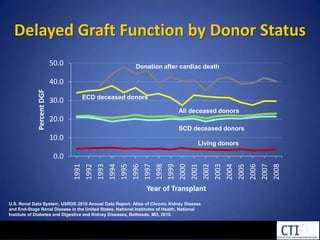
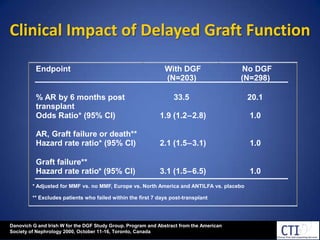
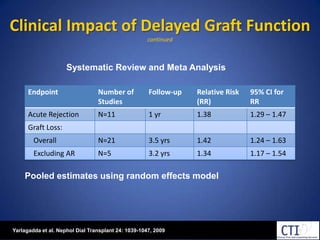
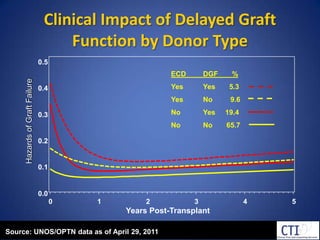
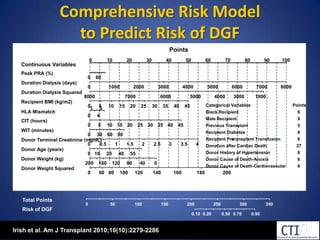
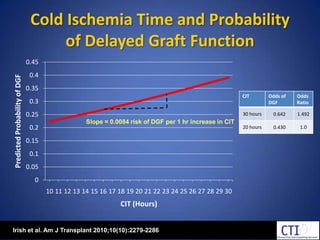
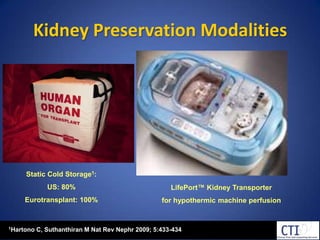
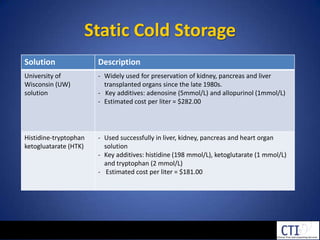
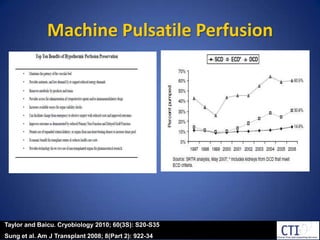
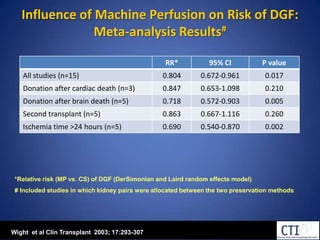
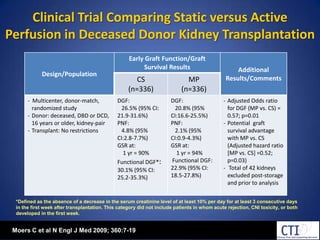
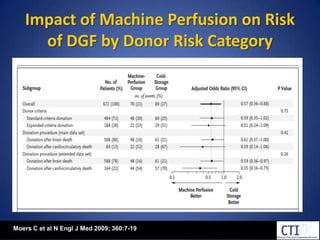
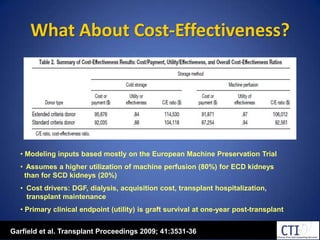
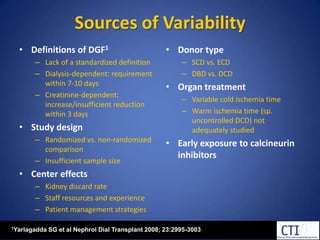
This document discusses cold machine perfusion versus static cold storage for preserving kidneys from standard criteria, extended criteria, and donation after cardiac death donors for transplantation. It summarizes the incidence and impact of delayed graft function, outlines kidney preservation methods and clinical trials comparing outcomes between cold storage and machine perfusion. It identifies unanswered questions around how preservation method may differentially impact outcomes based on donor and recipient risk factors.


















![Human Renal Transplantation [Dr. Edmond Wong]](https://cdn.slidesharecdn.com/ss_thumbnails/humanrenaltransplantationedmond-140716214736-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)































