Downloaded 24 times
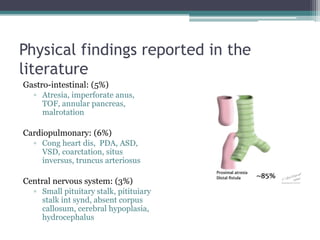
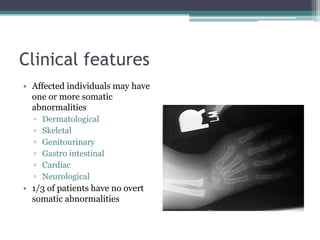

Fanconi anemia is a rare genetic disorder characterized by bone marrow failure and cancer predisposition. It results from defects in DNA interstrand crosslink repair. The disease was first described in 1927 and shows considerable genetic and clinical heterogeneity. Patients have physical abnormalities and bone marrow failure. The main risks are aplastic anemia, leukemia, and solid tumors. Treatment involves blood transfusions, androgens, and hematopoietic stem cell transplant. Management aims to prevent complications and cancers through surveillance and timely intervention.































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)













