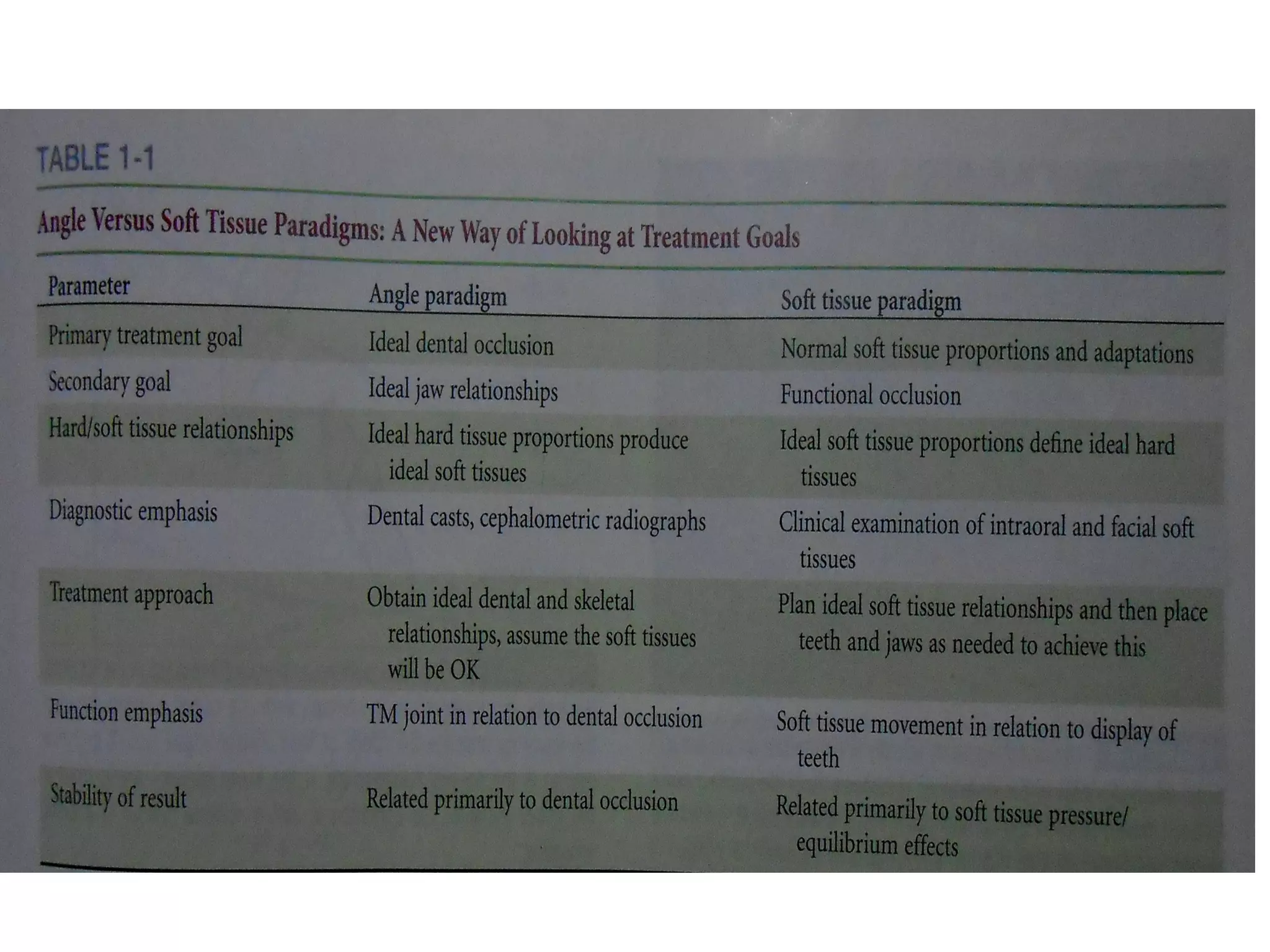
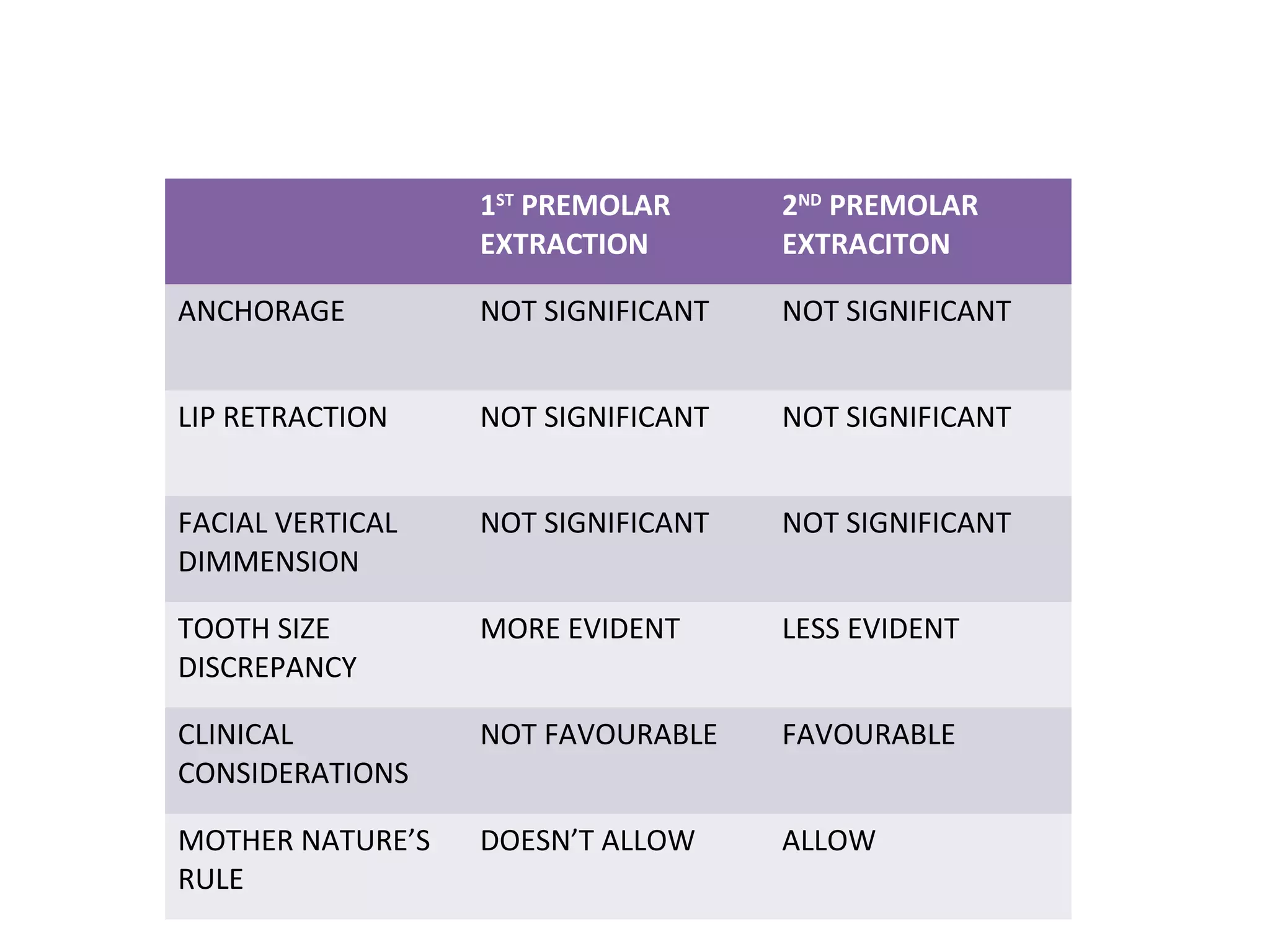
This document discusses extraction vs non-extraction in orthodontic treatment. It provides an overview of the history of extractions in orthodontics from ancient times to modern trends. Key factors in determining whether extractions are needed include facial analysis, soft tissue profile, midline, growth status, model analysis using Carey's analysis and Curve of Spee, and cephalometric measurements of vertical proportions and lower incisor position. Common teeth considered for extraction include premolars, canines, and molars, with specific indications outlined for each.