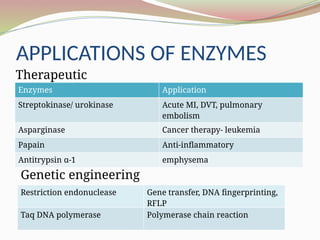
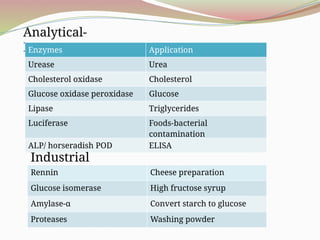
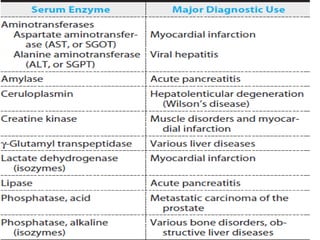
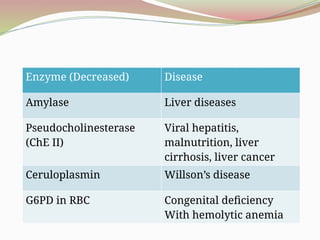
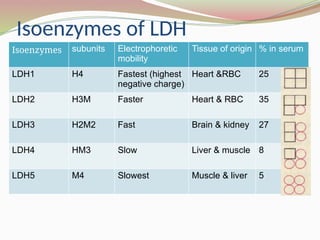
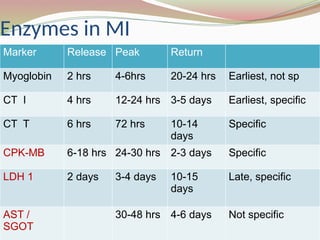
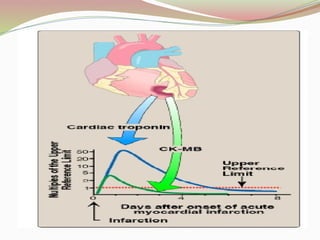
The document discusses various applications of enzymes in medical diagnostics, treatment, and industrial processes. It highlights the significance of plasma and non-plasma specific enzymes in diagnosing diseases, such as liver conditions, cancer, and myocardial infarction. Additionally, it covers isoenzymes, their characteristics, and how enzyme levels can indicate specific health issues.