This document provides an overview of endodontic sealers, including their history, classification, composition, and properties. It discusses various types of sealers such as zinc oxide-eugenol based sealers, resin based sealers, and calcium hydroxide containing sealers. The document also covers the mechanisms of setting for different sealers and reviews their ability to provide a fluid-tight seal in the root canal system.





![2. Salicylate-based sealers
• Salicylate-based sealers are referred by their marketed
therapeutic additives instead of their composition.
• For example, Sealapex (Kerr) and Apexit/ Apexit Plus (Ivoclar
Vivadent, Schaan, Lichtenstein) are examples of a calcium-
hydroxide-containing salicylate sealers.
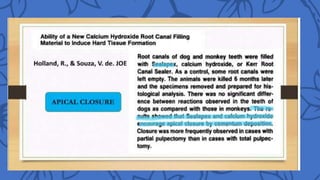
• Calcium hydroxide [Ca(OH)2] is both alkaline and antimicrobial,
desirable qualities for a therapeutic sealer.](https://image.slidesharecdn.com/endodonticsealers1-240407091043-4eb0abc6/85/ENDODONTIC-SEALERS-CLASSIFICATION-AND-TYPES-pptx-32-320.jpg)
![• Gutta percha milled to a low grain size is mixed into components of the
silicone sealer [Gutta-flow (Coltene Dental, USA)].
• It has extraordinary chemical and physical properties that offer maximum
sealing quality and biocompatibility.
• It contains small gutta-percha particles with a size of <30μ as filler.
• The material is flowable and sets within 10 min.
• The material flows into the smallest dentinal tubules, because of the small
particle size (<0.9 μm) of the GuttaFlow matrix filler.](https://image.slidesharecdn.com/endodonticsealers1-240407091043-4eb0abc6/85/ENDODONTIC-SEALERS-CLASSIFICATION-AND-TYPES-pptx-44-320.jpg)