Cortisol:
• At least95% of the glucocorticoid activity results from the secretion of cortisol.
• Function:
1) Cortisol may improve cardiac function by increasing the number or responsiveness of
beta-adrenergic receptors.
2) Developmental Changes: Plasma concentrations of cortisol increase progressively
during the last trimester of pregnancy.
3) Gluconeogenesis: Amino acids are mobilized from extrahepatic sites and transferred to
the liver for conversion to glucose
4) Protein Catabolism: Cortisol breaks down protein stores in nearly all cells except
hepatocytes, to mobilize amino acids for gluconeogenesis.
5) Antiinflammatory Effect:cortisol stabilizes lysosomal membranes, stops migration of
leukocytes into the infl amed area
4.
Aldosterone :
• Aldosteroneaccounts for approximately 95% of the
mineralocorticoid activity of the corticosteroids.
• Aldosterone sustains extracellular fluid volume by
conserving sodium and by maintaining a normal plasma
concentration of potassium.
5.
ADRENAL GLAND
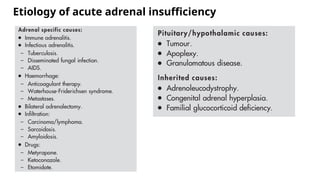
1. AddisonianCrisis
• It is a life threatening medical emergency of decompensated adrenal
insufficiency presents with hypotension and acute circulatory failure.
• Adrenal insu ciency (AI) can result from :
ffi
a) Primary Adrenal insufficiency
b) Secondary Adrenal insufficiency
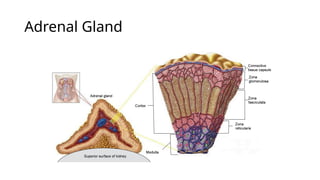
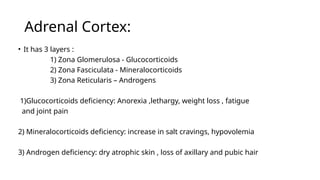
Adrenal Cortex:
• Ithas 3 layers :
1) Zona Glomerulosa - Glucocorticoids
2) Zona Fasciculata - Mineralocorticoids
3) Zona Reticularis – Androgens
1)Glucocorticoids deficiency: Anorexia ,lethargy, weight loss , fatigue
and joint pain
2) Mineralocorticoids deficiency: increase in salt cravings, hypovolemia
3) Androgen deficiency: dry atrophic skin , loss of axillary and pubic hair
8.
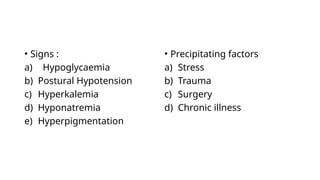
• Signs :
a)Hypoglycaemia
b) Postural Hypotension
c) Hyperkalemia
d) Hyponatremia
e) Hyperpigmentation
• Precipitating factors
a) Stress
b) Trauma
c) Surgery
d) Chronic illness
10.
Management:
• Hydrocortisone 100mg intravenously, followed by 50mg every 6th
hourly for 24 hours
is given.
• Fludrocortisone 50- 100mcg can be added if mineralocorticoid deficiency is present.
• Once the patient is recovering, the dose of hydrocortisone can be gradually tapered from
second day.
• Fluids and electrolytes replacement is done as indicated by vital signs and serum
electrolyte levels.
11.
Steroid replacement therapyin
unstressed patient :
• Glucocorticoid replacement:
Prednisolone 5mg in the morning and 2.5mg in the
evening
Or
Hydrocortisone 20mg in the morning and 10mg in the
evening
• Mineralocorticoid replacement:
Fludrocortisone – 0.05 to 0.1 mg / day
12.
Anaesthetic Considerations ina crisis or
surgical stress:
Management options for steroid replacement in
perioperative period based on degree of surgical stress:
• For minor surgeries: Give usual morning dose of steroid
and no supplement is needed.
• For Moderate surgeries: Give usual morning dose of
steroid and administer 50mg of Hydrocortisone IV prior to
induction and 25mg every 8th
hourly for 24 to 36 hrs.
• For Major Surgeries: Give usual morning dose of steroid
and administer 100mg of Hydrocortisone IV prior to
induction and 50mg every 8th
hourly for 24 to 36 hrs.
13.
2.Cushing syndrome
• Cushingsyndrome is a clinical condition caused by
prolonged exposure to excess glucocorticoids (cortisol) from
any source produced endogenously in the body (as in
adrenal or pituitary tumors) or administered exogenously
(long-term steroid therapy)
• Cushing’s disease accounts for 70% of patients with
endogenous causes of Cushing syndrome
14.
Pathophysiology
• Cortisol actsas a precursor for cortisone synthesis
• 11β hydroxy steroid dehydrogenase type 2 enzyme is used
in producing cortisone.
• Defect or decrease in 11β hsd type 2 levels leads to
hypercortisolism condition.
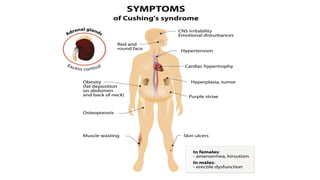
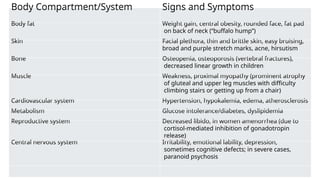
Body Compartment/System Signsand Symptoms
Body fat Weight gain, central obesity, rounded face, fat pad
on back of neck (“buffalo hump”)
Skin Facial plethora, thin and brittle skin, easy bruising,
broad and purple stretch marks, acne, hirsutism
Bone Osteopenia, osteoporosis (vertebral fractures),
decreased linear growth in children
Muscle Weakness, proximal myopathy (prominent atrophy
of gluteal and upper leg muscles with difficulty
climbing stairs or getting up from a chair)
Cardiovascular system Hypertension, hypokalemia, edema, atherosclerosis
Metabolism Glucose intolerance/diabetes, dyslipidemia
Reproductive system Decreased libido, in women amenorrhea (due to
cortisol-mediated inhibition of gonadotropin
release)
Central nervous system Irritability, emotional lability, depression,
sometimes cognitive defects; in severe cases,
paranoid psychosis
19.
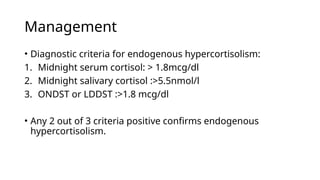
Management
• Diagnostic criteriafor endogenous hypercortisolism:
1. Midnight serum cortisol: > 1.8mcg/dl
2. Midnight salivary cortisol :>5.5nmol/l
3. ONDST or LDDST :>1.8 mcg/dl
• Any 2 out of 3 criteria positive confirms endogenous
hypercortisolism.
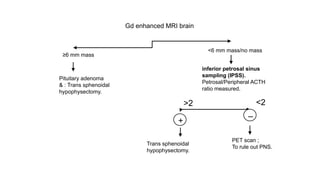
Gd enhanced MRIbrain
≥6 mm mass
<6 mm mass/no mass
Trans sphenoidal
hypophysectomy.
PET scan ;
To rule out PNS.
Pituitary adenoma
& : Trans sphenoidal
hypophysectomy.
inferior petrosal sinus
sampling (IPSS).
Petrosal/Peripheral ACTH
ratio measured.
+
–
>2 <2
22.
3. PHEOCHROMOCYTOMA
• Pheochromocytomais a condition in which neural crest cells produce catecholamines
and catecholamine metabolites
• Crisis is caused by the action of unopposed high circulating levels of catecholamines
acting at adrenoreceptors:
• a-receptors cause a pressor response with increases in blood pressure, while b-receptor
activation has positive inotropic and chronotropic effects.
• Release of catecholamines from phaeochromocytoma may be episodic.
• Based onorigin pheochromocytoma is divided into two types:
A) Adrenal pheochromocytoma: Adrenaline >Noradrenaline
B) Extra adrenal pheochromocytoma: produce only Noradrenaline
Currently
• Rule of 10 : 10% familial. 40% familial
10% Extraadrenal. 25% extra adrenal
10% bilateral 40% Bilateral
10% malignant. 50% malignant
25.
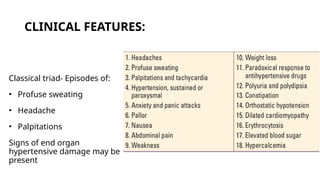
CLINICAL FEATURES:
Classical triad-Episodes of:
• Profuse sweating
• Headache
• Palpitations
Signs of end organ
hypertensive damage may be
present
26.
Diagnosis of pheochromocytoma
•Investigations:
a)Biochemical tests;
1) 24 hour urine fractionated metanephrines
Or nor metanephrines
2) Plasma fractionated metanephrines or
nor metanephrines
b) Imaging: 1) MRI abdomen
2) MIBG
3) FDG PET scan
4) Gallium DOTATATE PET scan – IOC for patients with biochemical
test positive and MRI is negative.
27.
Treatment:
• Therapy shouldnot wait for biochemical confirmation.
• The non-competitive a1 >a 2 antagonist Phenoxybenzamine is the drug of choice
with a starting dose of 10 mg orally three times a day.
• Oral prazosin or intravenous phentolamine can be used to manage paroxysms
while adequate alpha blockade is awaited.
• After the first 48 hours, propanolol 40 mg orally three times a day may be added.
28.
Important pharmacological issuesin
treatment
• It is vital that 48 hours of a-blockade precede b-blockade to avoid
exacerbating a crisis through the unopposed action of catecholamines at
a-receptors.
• Side effects to be expected include postural hypotension, nasal
stuffiness, drowsiness, and dilutional anaemia.
• The use of labetalol is not recommended as this has relatively greater b-
blocking action compared to its a-blocking action, and hence can even
precipitate or worsen phaeochromocytoma crisis.
29.
Surgical treatment forpheochromocytoma
• Laparoscopic retro peritoneal adrenalectomy is the treatment
of choice for pheochromocytoma.
30.
Anaesthetic considerations:
Preopertive preparation:
•Phenoxybenzamine a long acting ,non competitive, α- 1 and α-
2 antagonist given 10 mg 8th
hrly.
• Most of the patients need 80-200mg in a day.
• α blockade therapy should be started 10 to 14days before
proposed surgery.
• Calcium channel blockers can also be used alone or along with
α blockers.
• Beta blockers can be started only after adequate α blockade
occurs.
31.
• α-Methyltyrosine isreserved for patients with metastatic
disease or for situations in which surgery is contraindicated.
• When α-methyltyrosine is used in combination with
αadrenergic–blocking agents, there is a significant reduction
in catecholamine synthesis.
• In pregnant woman , trend is to perform surgery during the
first trimester or at the time of cesarean delivery.
32.
Perioperative considerations :
•Symptomatic patients continue to receive medical therapy until tachycardia,
cardiac dysrhythmias, and paroxysmal elevations in blood pressure are well
controlled.
• If patient is not undergone preop treatment, it may be necessary to infuse
nitroprusside during the induction of anesthesia.
• A low-dose infusion is often initiated in anticipation of the marked blood
pressure elevations that can occur with laryngoscopy and surgical stimulus.
• A sedative–hypnotic, in combination with an opioid analgesic, is often selected
for induction
33.
• It isextremely important to achieve an adequate depth of anesthesia
before proceeding with laryngoscopy to minimize the sympathetic
nervous system response to this maneuver.
• Manipulation of the tumor may produce a marked elevation in blood
pressure. Acute hypertensive crises are treated with IV infusions of
nitroprusside or phentolamine
• The reduction in blood pressure that may occur after ligation of the
tumor’s venous supply should be anticipated.
34.
Post operative considerations:
•After surgery, catecholamine levels return to normal over several
days(within 10 days in 75% of people )
• Hypoglycemia must be watched because, as insulin levels rise
from loss of catecholamine-induced β-cell suppression.
35.
PANCREAS
A. Diabetic Ketoacidosis:
•Diabetic ketoacidosis is a medical emergency and a serious complication
of diabetes. More common and marked in type 1 DM and rare and may
also occur in type 2 DM
• Major three biochemical features of DKA:
1) Hyperglycemia
2) Hyperketonemia( and ketonuria)
3) Metabolic acidosis
• Consequences of insulin deficiency and glucagon excess is severe
hyperglycemia, diuresis and dehydration
36.
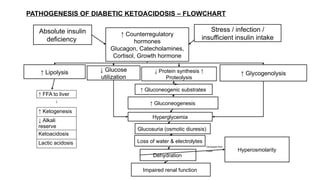
Absolute insulin
deficiency
↑ Counterregulatory
hormones
Glucagon,Catecholamines,
Cortisol, Growth hormone
↓ Glucose
utilization
↑ Lipolysis ↓ Protein synthesis ↑
Proteolysis
↑ Glycogenolysis
↑ FFA to liver
↓
↑ Ketogenesis
↓ Alkali
reserve
Ketoacidosis
Lactic acidosis
↑ Gluconeogenic substrates
↑ Gluconeogenesis
Hyperglycemia
Glucosuria (osmotic diuresis)
Loss of water & electrolytes
Dehydration
Impaired renal function
Hyperosmolarity
Decreased fluid
intake
PATHOGENESIS OF DIABETIC KETOACIDOSIS – FLOWCHART
Stress / infection /
insufficient insulin intake
37.
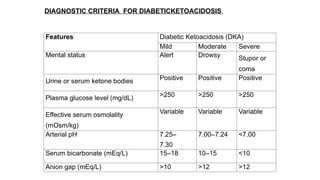
DIAGNOSTIC CRITERIA FORDIABETICKETOACIDOSIS
Features Diabetic Ketoacidosis (DKA)
Mild Moderate Severe
Mental status Alert Drowsy Stupor or
coma
Urine or serum ketone bodies Positive Positive Positive
Plasma glucose level (mg/dL) >250 >250 >250
Effective serum osmolality
(mOsm/kg)
Variable Variable Variable
Arterial pH 7.25–
7.30
7.00–7.24 <7.00
Serum bicarbonate (mEq/L) 15–18 10–15 <10
Anion gap (mEq/L) >10 >12 >12
38.
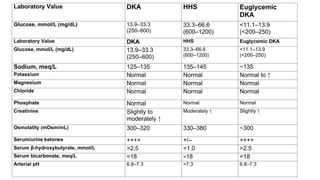
Laboratory Value DKAHHS Euglycemic
DKA
Glucose, mmol/L (mg/dL) 13.9–33.3
(250–600)
33.3–66.6
(600–1200)
<11.1–13.9
(<200–250)
Laboratory Value DKA HHS Euglycemic DKA
Glucose, mmol/L (mg/dL) 13.9–33.3
(250–600)
33.3–66.6
(600–1200)
<11.1–13.9
(<200–250)
Sodium, meq/L 125–135 135–145 ~135
Potassium Normal Normal Normal to ↑
Magnesium Normal Normal Normal
Chloride Normal Normal Normal
Phosphate Normal Normal Normal
Creatinine Slightly to
moderately ↑
Moderately ↑ Slightly ↑
Osmolality (mOsm/mL) 300–320 330–380 ~300
Serum/urine ketones ++++ +/– ++++
Serum β-hydroxybutyrate, mmol/L >2.5 <1.0 >2.5
Serum bicarbonate, meq/L <18 >18 <18
Arterial pH 6.8–7.3 >7.3 6.8–7.3
39.
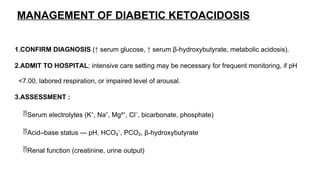
MANAGEMENT OF DIABETICKETOACIDOSIS
1.CONFIRM DIAGNOSIS (↑ serum glucose, ↑ serum β-hydroxybutyrate, metabolic acidosis).
2.ADMIT TO HOSPITAL; intensive care setting may be necessary for frequent monitoring, if pH
<7.00, labored respiration, or impaired level of arousal.
3.ASSESSMENT :
Serum electrolytes (K⁺, Na⁺, Mg²⁺, Cl⁻, bicarbonate, phosphate)
Acid–base status — pH, HCO₃⁻, PCO₂, β-hydroxybutyrate
Renal function (creatinine, urine output)
40.
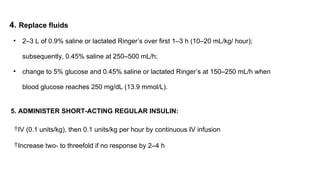
4. Replace fluids
•2–3 L of 0.9% saline or lactated Ringer’s over first 1–3 h (10–20 mL/kg/ hour);
subsequently, 0.45% saline at 250–500 mL/h;
• change to 5% glucose and 0.45% saline or lactated Ringer’s at 150–250 mL/h when
blood glucose reaches 250 mg/dL (13.9 mmol/L).
5. ADMINISTER SHORT-ACTING REGULAR INSULIN:
IV (0.1 units/kg), then 0.1 units/kg per hour by continuous IV infusion
Increase two- to threefold if no response by 2–4 h
41.
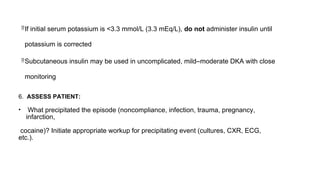
If initial serumpotassium is <3.3 mmol/L (3.3 mEq/L), do not administer insulin until
potassium is corrected
Subcutaneous insulin may be used in uncomplicated, mild–moderate DKA with close
monitoring
6. ASSESS PATIENT:
• What precipitated the episode (noncompliance, infection, trauma, pregnancy,
infarction,
cocaine)? Initiate appropriate workup for precipitating event (cultures, CXR, ECG,
etc.).
42.
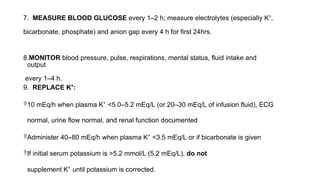
7. MEASURE BLOODGLUCOSE every 1–2 h; measure electrolytes (especially K⁺,
bicarbonate, phosphate) and anion gap every 4 h for first 24hrs.
8.MONITOR blood pressure, pulse, respirations, mental status, fluid intake and
output
every 1–4 h.
9. REPLACE K⁺:
10 mEq/h when plasma K⁺ <5.0–5.2 mEq/L (or 20–30 mEq/L of infusion fluid), ECG
normal, urine flow normal, and renal function documented
Administer 40–80 mEq/h when plasma K⁺ <3.5 mEq/L or if bicarbonate is given
If initial serum potassium is >5.2 mmol/L (5.2 mEq/L), do not
supplement K⁺ until potassium is corrected.
43.
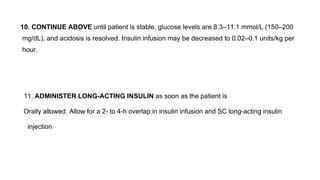
10. CONTINUE ABOVEuntil patient is stable, glucose levels are 8.3–11.1 mmol/L (150–200
mg/dL), and acidosis is resolved. Insulin infusion may be decreased to 0.02–0.1 units/kg per
hour.
11. ADMINISTER LONG-ACTING INSULIN as soon as the patient is
Orally allowed. Allow for a 2- to 4-h overlap in insulin infusion and SC long-acting insulin
injection
44.
References:
• Harrison’s principlesof internal medicine 21st edition
• Clinical Anesthesia by Paul G Barasch
• STOELTING’S HANDBOOK OF Pharmacology and Physiology in Anesthetic Practice

































![Polymer [ बहुलक ] Chemistry Notes PDF - Irfanullah Mehar - JJ Sir Chemistry.pdf](https://cdn.slidesharecdn.com/ss_thumbnails/polymerchemistrynotespdf-irfanullahmehar-jjsirchemistry-260210172118-3f9b37f7-thumbnail.jpg?width=640&height=640&fit=bounds)
















