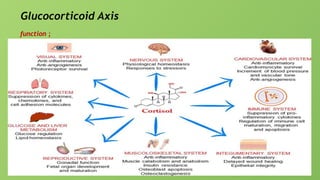
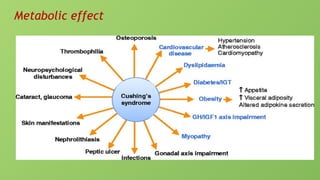
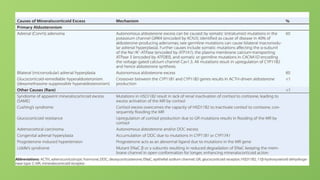
1- Cushing syndrome
prevalence
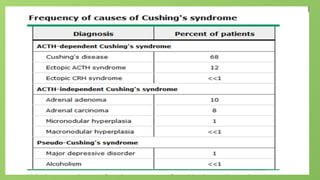
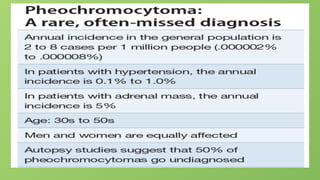
Anestimated 10-15 per million people are affected every year. Pituitary
adenomas (Cushing's disease) account for more than 70 percent of cases in adults
and about 60-70 percent of cases in children and adolescents.
In iatrogenic Cushing the prevalence was 7.6%
Pseudo Cushing
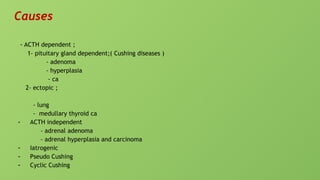
Causes ;
-obesity
- depression
- alcohol
Iatrogenic Cushing syndrome
clinical features
- symptoms and sign suggestive of Cushing
- symptoms and sign suggestive of adrenal insufficiency
Cyclic Cushing
Definition
Cyclic Cushing's syndrome (CS) is a rare disorder, characterized by repeated episodes of cortisol excess interspersed by
periods of normal cortisol secretion. The so-called cycles of hypercortisolism can occur regularly or irregularly with
intercyclic phases ranging from days to years
Causes
- Hypothalamic factors
- Feed back mechanism
- Tumor infarction
11.
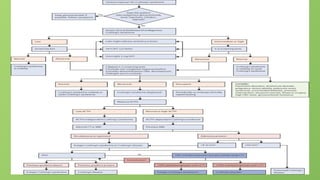
Diagnosis of Cushingsyndrome
A- criteria for diagnosis
1- late night or salivary cortisone
2- 24 h urinary free cortisol
3- overnight dexamethasone suppression test
B- Investigation to know the type ;
- is it Cushing syndrome
- diagnosis of pseudo Cushing
overnight dexamethasone suppression test
and or low dose
- diagnosis of iatrogenic Cushing
If you use cortisone, prednisone, or other corticosteroids, the following test results may suggest exogenous Cushing syndrome:
Low ACTH level
Low cortisol level (or high cortisol level) in the blood or urine, depending on the medicine you are taking
Abnormal response to a cosyntropin (ACTH) stimulation test
Higher than normal fasting glucose level
Low blood potassium level
Low bone density, as measured by bone mineral density test
High cholesterol, particularly high triglycerides and low high-density lipoprotein (HDL)
A method called high performance liquid chromatography (HPLC) can show a high level of the suspected medicine in the urine.
12.
If cushing syndromeis diagnosed
A- investigation to know the type
- ACTH dependent
by measurement of ACTH
If its height ;
so its ACTH dependent
- if its ACTH dependent do investigation to know if its pituitary or ectopic
- Clinical
- Laboratory:
- serum K
- high dose dexamethasone suppression test
- inferior petrosal sinus sample with and without CRH test
If its low ; so its ACTH indepedents
- check for serum cortisol
- androgen
13.
Imaging
- MRI ofpituitary gland
- MRI of chest
Diagnosis of ACTH independent
Laboratory
- measurement of cortisol
- measurement of CRH
diagnosis of cyclic Cushing syndrome Patients who fulfilled the following conditions were
diagnosed with CCS: (1) The patient exhibited at least three peaks and two valleys in cortisol
levels (the peaks should exceed the upper limit of normal) to diagnose CCS [5]. (2) The patient
had clinical symptoms of CS, which can spontaneously disappear or recur. (3) Imaging studies
showed adrenal, pituitary, or ectopic lesions. (4) Patients did not use exogenous hormones and
did not have simple obesity, autonomous cortisol secretion, pseudo-CS, or glucocorticoid-
resistant syndrome
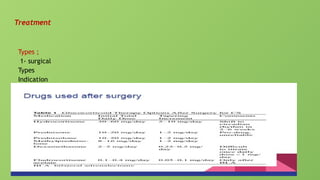
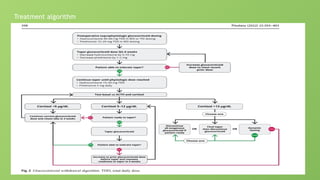
Treatment of iatrogenic
Treatmentis to decrease and eventually stop taking any corticosteroids. This may be done
slowly or quickly, depending on why you are being treated with corticosteroid. Do not stop
taking any medicine without first talking to your provider. Suddenly stopping corticosteroids
after taking them for a long time (usually more than 2 weeks) can result in a life-threatening
condition called adrenal crisis.
If you cannot stop taking the medicine because of disease (for example, you need glucocorticoid
medicine to treat severe asthma), follow your provider's instructions on how to reduce the
possibility of developing complications, including:
Treating high blood sugar with diet, oral medicines, or insulin.
Treating high cholesterol with diet or medicines.
Taking medicines to prevent bone loss. This can help reduce the risk for fractures if you
develop osteoporosis.
Taking other medicines to decrease the amount of glucocorticoid medicine that you need.
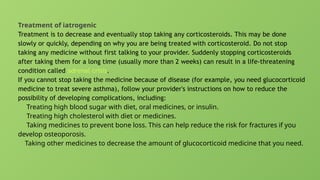
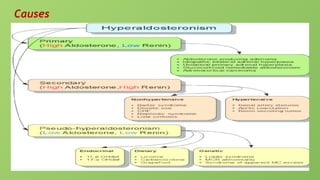
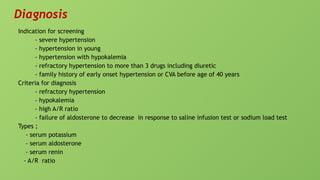
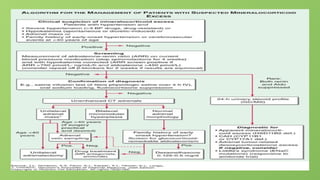
Diagnosis
Indication for screening
-severe hypertension
- hypertension in young
- hypertension with hypokalemia
- refractory hypertension to more than 3 drugs including diuretic
- family history of early onset hypertension or CVA before age of 40 years
Criteria for diagnosis
- refractory hypertension
- hypokalemia
- high A/R ratio
- failure of aldosterone to decrease in response to saline infusion test or sodium load test
Types ;
- serum potassium
- serum aldosterone
- serum renin
- A/R ratio
27.
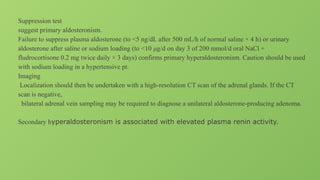
Suppression test
suggest primaryaldosteronism.
Failure to suppress plasma aldosterone (to <5 ng/dL after 500 mL/h of normal saline × 4 h) or urinary
aldosterone after saline or sodium loading (to <10 μg/d on day 3 of 200 mmol/d oral NaCl +
fludrocortisone 0.2 mg twice daily × 3 days) confirms primary hyperaldosteronism. Caution should be used
with sodium loading in a hypertensive pt.
Imaging
Localization should then be undertaken with a high-resolution CT scan of the adrenal glands. If the CT
scan is negative,
bilateral adrenal vein sampling may be required to diagnose a unilateral aldosterone-producing adenoma.
Secondary hyperaldosteronism is associated with elevated plasma renin activity.
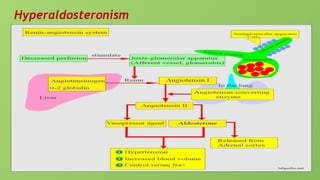
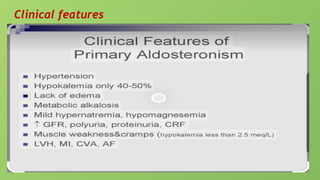
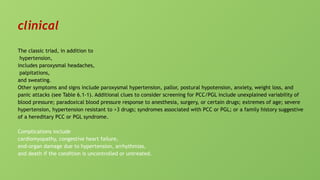
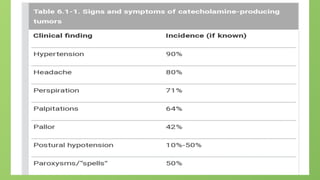
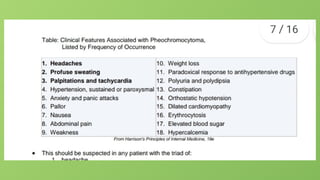
clinical
The classic triad,in addition to
hypertension,
includes paroxysmal headaches,
palpitations,
and sweating.
Other symptoms and signs include paroxysmal hypertension, pallor, postural hypotension, anxiety, weight loss, and
panic attacks (see Table 6.1-1). Additional clues to consider screening for PCC/PGL include unexplained variability of
blood pressure; paradoxical blood pressure response to anesthesia, surgery, or certain drugs; extremes of age; severe
hypertension, hypertension resistant to >3 drugs; syndromes associated with PCC or PGL; or a family history suggestive
of a hereditary PCC or PGL syndrome.
Complications include
cardiomyopathy, congestive heart failure,
end-organ damage due to hypertension, arrhythmias,
and death if the condition is uncontrolled or untreated.
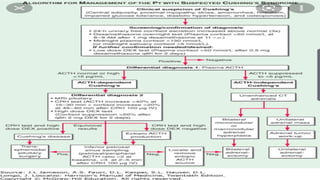
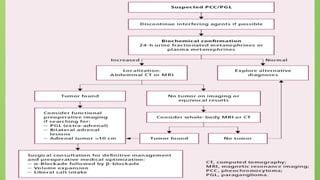
36.
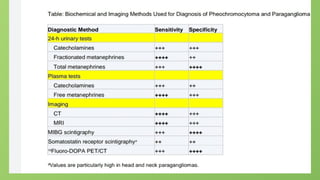
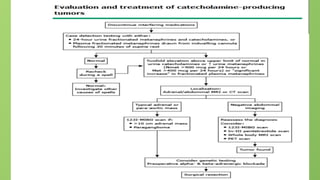
investigation
Screening
Screening should beconsidered in patients with suggestive clinical features (see above). It
should also be considered if there is an incidentally discovered adrenal or retroperitoneal mass
with ≥10 Hounsfield unit attenuation on unenhanced computed tomography (CT) or low
washout on a contrast-enhanced study, or if the patient is known to be a carrier of disease-
causing genetic mutations of syndromes (eg, mutations in RET [MEN 2, MEN 3], VHL, SDHx, or
NF1 genes).
37.
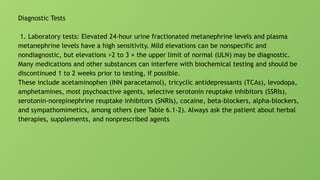
Diagnostic Tests
1. Laboratorytests: Elevated 24-hour urine fractionated metanephrine levels and plasma
metanephrine levels have a high sensitivity. Mild elevations can be nonspecific and
nondiagnostic, but elevations >2 to 3 × the upper limit of normal (ULN) may be diagnostic.
Many medications and other substances can interfere with biochemical testing and should be
discontinued 1 to 2 weeks prior to testing, if possible.
These include acetaminophen (INN paracetamol), tricyclic antidepressants (TCAs), levodopa,
amphetamines, most psychoactive agents, selective serotonin reuptake inhibitors (SSRIs),
serotonin-norepinephrine reuptake inhibitors (SNRIs), cocaine, beta-blockers, alpha-blockers,
and sympathomimetics, among others (see Table 6.1-2). Always ask the patient about herbal
therapies, supplements, and nonprescribed agents
40.
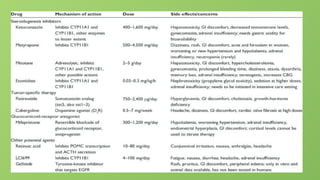
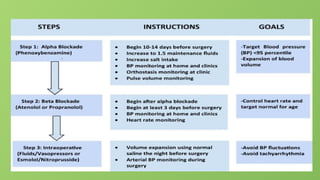
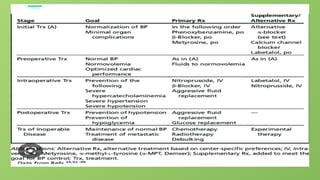
1- preparation forsurgery
- use of antihypertensive drugs
- proper hydration generous fluid and sodium intake.
Treatment target ; Target blood pressure should be in the low-normal range for age (<130/80
mm Hg and systolic blood pressure [SBP] >110 mm Hg in a standing position), while avoiding
significant orthostatic hypotension or its symptoms.
Treatment types Optimal blood pressure control with combined alpha- and beta-blockade is
essential prior to planned surgery along with adequate hydration with It is important to use
alpha-blockade first, starting at least 10 to 14 days before surgery, and then follow with beta-
blockade 3 to 4 days later (for controlling the risk of tachycardia and arrhythmia) to mitigate
unopposed alpha-receptor stimulation, which could lead to catastrophic hypertension and
cardiopulmonary decompensation.
41.
1-Alpha-adrenergic blockade: Anonselective alpha-blocker may be used, for instance,
phenoxybenzamine 10 mg bid as a starting dose and titrated up to 60 mg bid. Alternatively, a
selective alpha-1 adrenergic blocker such as doxazosin at a starting dose of 1 to 2 mg daily and
titrated up to 16 mg bid may be used.
2) Beta-adrenergic blockade: Beta-blocker therapy is used to control tachycardia. Beta-
blockers should be initiated a few days after adequate blood pressure control has been
achieved with alpha-blockade to attain a target heart rate of 60 to 80 beats per minute
44.
Surgery:
1) PCC: Laparoscopiclocalized adrenalectomy by an experienced adrenal surgeon may be
done for the majority of patients, especially if a small, unilateral, intra-adrenal tumor with
nonmalignant features is found on imaging. Other patients may require open laparotomy.
2) PGL requires resection by a surgeon experienced in the particular site(s) where the tumor
is located

![Imaging
- MRI of pituitary gland
- MRI of chest
Diagnosis of ACTH independent
Laboratory
- measurement of cortisol
- measurement of CRH
diagnosis of cyclic Cushing syndrome Patients who fulfilled the following conditions were
diagnosed with CCS: (1) The patient exhibited at least three peaks and two valleys in cortisol
levels (the peaks should exceed the upper limit of normal) to diagnose CCS [5]. (2) The patient
had clinical symptoms of CS, which can spontaneously disappear or recur. (3) Imaging studies
showed adrenal, pituitary, or ectopic lesions. (4) Patients did not use exogenous hormones and
did not have simple obesity, autonomous cortisol secretion, pseudo-CS, or glucocorticoid-
resistant syndrome](https://image.slidesharecdn.com/xxeanrjqqlygq8tv4c7n-adrenal-gland-hyperaldosteronism-2-250429145558-741220d8/85/adrenal_gland_hyperaldosteronism-type-and-causes-13-320.jpg)

![investigation
Screening
Screening should be considered in patients with suggestive clinical features (see above). It
should also be considered if there is an incidentally discovered adrenal or retroperitoneal mass
with ≥10 Hounsfield unit attenuation on unenhanced computed tomography (CT) or low
washout on a contrast-enhanced study, or if the patient is known to be a carrier of disease-
causing genetic mutations of syndromes (eg, mutations in RET [MEN 2, MEN 3], VHL, SDHx, or
NF1 genes).](https://image.slidesharecdn.com/xxeanrjqqlygq8tv4c7n-adrenal-gland-hyperaldosteronism-2-250429145558-741220d8/85/adrenal_gland_hyperaldosteronism-type-and-causes-36-320.jpg)
![1- preparation for surgery
- use of antihypertensive drugs
- proper hydration generous fluid and sodium intake.
Treatment target ; Target blood pressure should be in the low-normal range for age (<130/80
mm Hg and systolic blood pressure [SBP] >110 mm Hg in a standing position), while avoiding
significant orthostatic hypotension or its symptoms.
Treatment types Optimal blood pressure control with combined alpha- and beta-blockade is
essential prior to planned surgery along with adequate hydration with It is important to use
alpha-blockade first, starting at least 10 to 14 days before surgery, and then follow with beta-
blockade 3 to 4 days later (for controlling the risk of tachycardia and arrhythmia) to mitigate
unopposed alpha-receptor stimulation, which could lead to catastrophic hypertension and
cardiopulmonary decompensation.](https://image.slidesharecdn.com/xxeanrjqqlygq8tv4c7n-adrenal-gland-hyperaldosteronism-2-250429145558-741220d8/85/adrenal_gland_hyperaldosteronism-type-and-causes-40-320.jpg)









































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)





![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)