
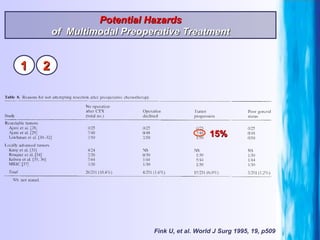
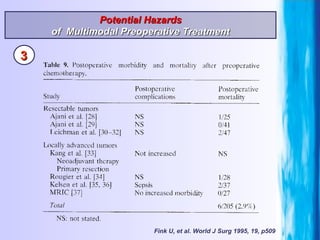
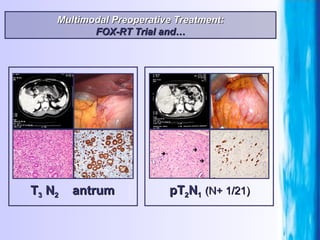
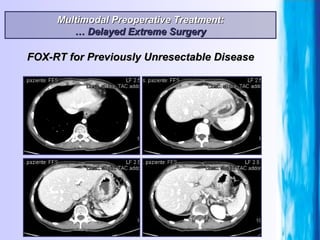

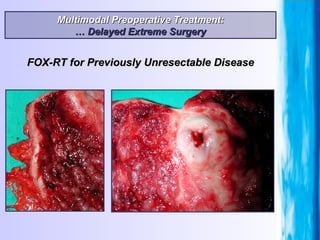
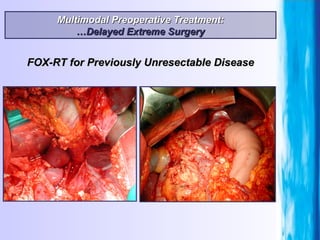

1) Multimodal preoperative treatment involving chemotherapy or chemoradiation before surgery can reduce the extent of gastric cancer and allow for complete resection in some patients who otherwise may have inoperable tumors. 2) While this approach can increase the chance of complete tumor removal, it also carries risks of treatment-related toxicity, tumor progression during treatment delay, and potential increases in postoperative complications. 3) Careful patient selection and standardization of surgical and pathological evaluation after preoperative treatment is important to maximize benefits and minimize hazards for gastric cancer patients undergoing a multimodal approach.























































































