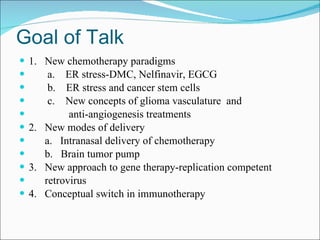
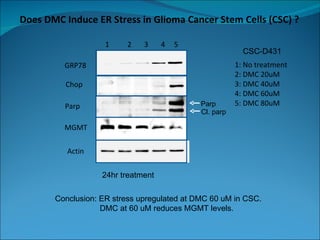
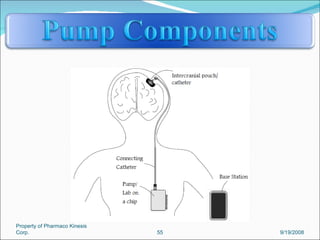
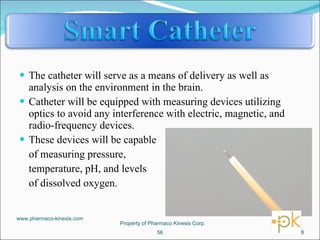
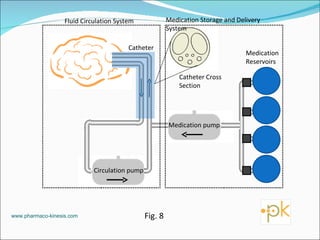
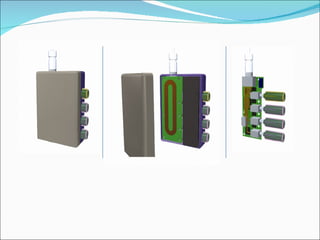
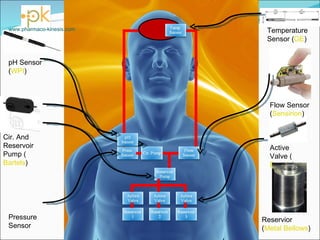
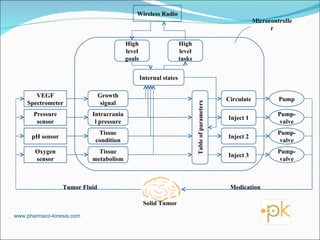
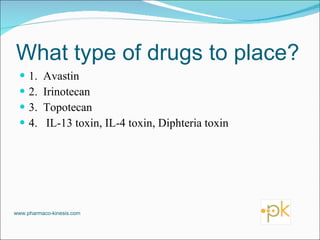
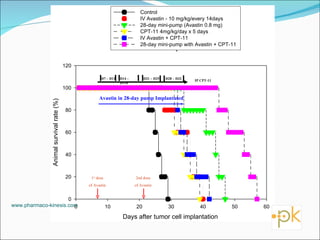
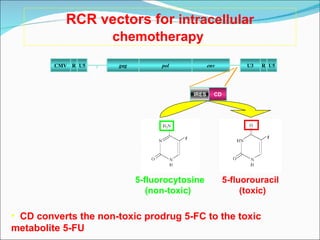
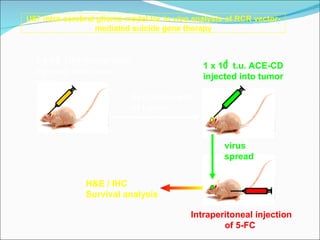
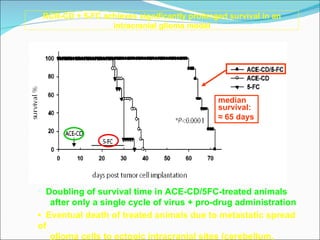
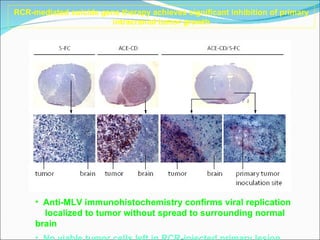
The document discusses new treatments being developed for malignant gliomas. It describes research into targeting the endoplasmic reticulum stress response pathway to induce apoptosis in glioma cells. Several new drug candidates and delivery methods are discussed, including an implantable pump being developed to provide continuous metronomic chemotherapy delivery directly to the brain tumor. Gene therapy using replication-competent retroviruses and improved immunotherapy approaches are also mentioned as promising new treatment strategies.