Failure to thrive in neonates and infants + pediatric case.pptx
Dm shoes criteria
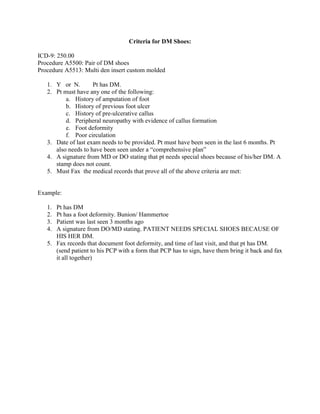
1. Criteria for DM Shoes:
ICD-9: 250.00
Procedure A5500: Pair of DM shoes
Procedure A5513: Multi den insert custom molded
1. Y or N.
Pt has DM.
2. Pt must have any one of the following:
a. History of amputation of foot
b. History of previous foot ulcer
c. History of pre-ulcerative callus
d. Peripheral neuropathy with evidence of callus formation
e. Foot deformity
f. Poor circulation
3. Date of last exam needs to be provided. Pt must have been seen in the last 6 months. Pt
also needs to have been seen under a “comprehensive plan”
4. A signature from MD or DO stating that pt needs special shoes because of his/her DM. A
stamp does not count.
5. Must Fax the medical records that prove all of the above criteria are met:
Example:
1.
2.
3.
4.
Pt has DM
Pt has a foot deformity. Bunion/ Hammertoe
Patient was last seen 3 months ago
A signature from DO/MD stating. PATIENT NEEDS SPECIAL SHOES BECAUSE OF
HIS HER DM.
5. Fax records that document foot deformity, and time of last visit, and that pt has DM.
(send patient to his PCP with a form that PCP has to sign, have them bring it back and fax
it all together)
2. I Dr.___________________________________________MD/DO am treating
______________________________________________, who has Diabetes Mellitus.
This patient needs special shoes (DEPTH
or CUSTOM MOLDED) because of his/her
Diabetes.
Signature of MD/DO___________________________________________________
(Stamped Signature Not Acceptable*)