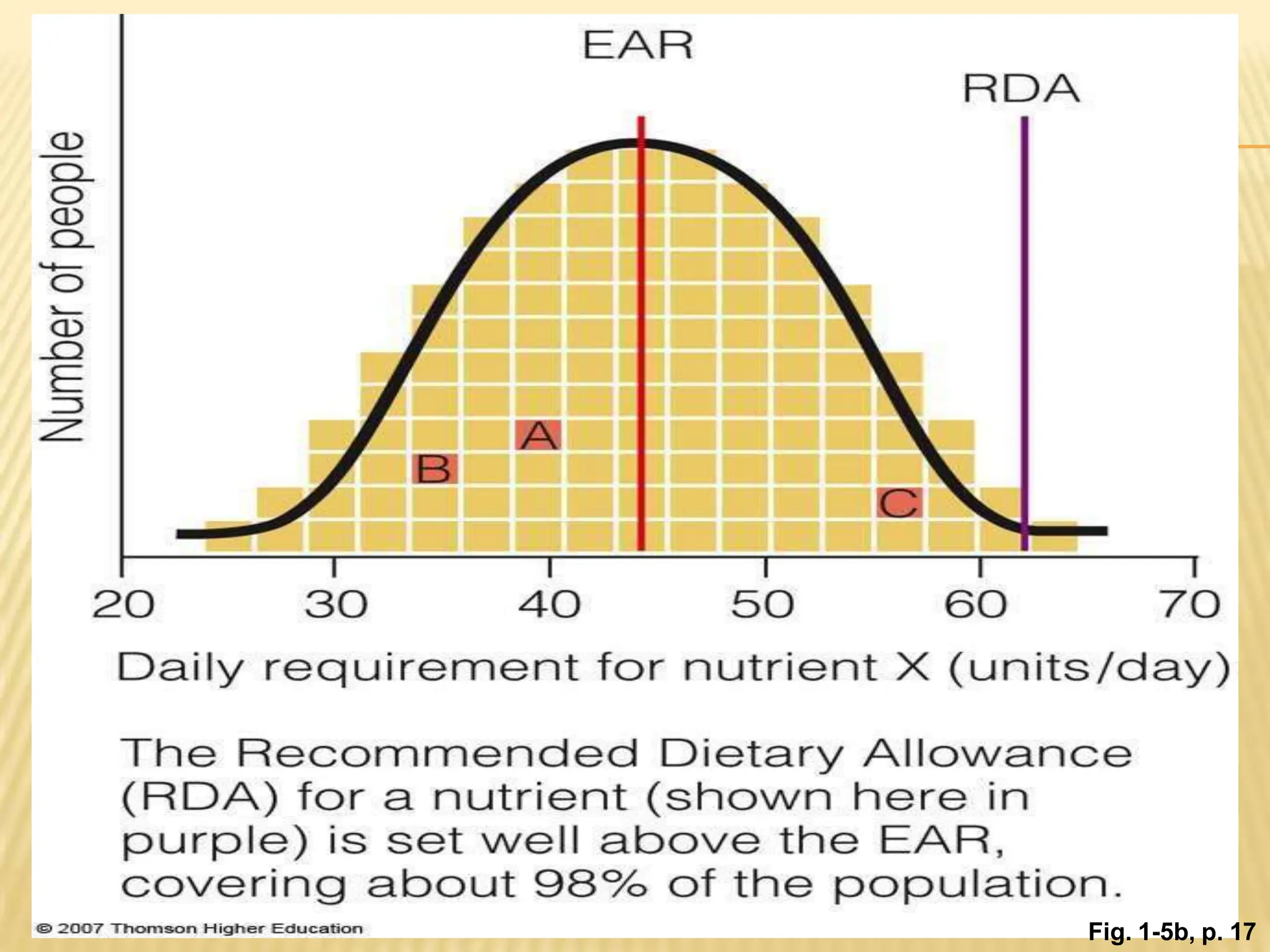
The DRI (Dietary Reference Intakes) are a set of nutrient standards that define nutrient amounts to support health. They are established by a committee that reviews thousands of studies. The standards include the EAR (Estimated Average Requirement), RDA (Recommended Dietary Allowance), AI (Adequate Intake), UL (Tolerable Upper Intake Level), and AMDR (Acceptable Macronutrient Distribution Range). The EAR is the daily intake amount estimated to meet nutrient needs in half the population. The RDA is set higher than the EAR to meet needs of nearly all people. The AI is used when data is insufficient to determine an EAR or RDA. Dietary assessment methods are used


![Estimated Energy Requirement (EER)
The energy recommendation—called the Estimated Energy
Requirement (EER)—represents the average dietary energy
intake (kcalories per day) that will maintain energy balance in
a person who has a healthy body weight ♦ and level of
physical activity. Balance is key to the energy
recommendation. Enough energy is needed to sustain a
healthy and active life, but too much energy can lead to weight
gain and obesity. Because any amount in excess of energy
needs will result in weight gain, no upper level for energy has
been determined.
Formula:Adult male: EER = 662 − [9.53 X age (y)] + PA X
[15.91 X wt (kg) + 539.6 X ht (m)]
Adult female: EER = 354 − [6.91 x age (y)] + PA x [9.36 x wt
(kg) + 726 x ht (m)]](https://image.slidesharecdn.com/dietaryreferanceintakedrilec4thsem-240221112757-aca71126/75/Dietary-Referance-Intake-DRI-Lec-4th-sem-pptx-13-2048.jpg)