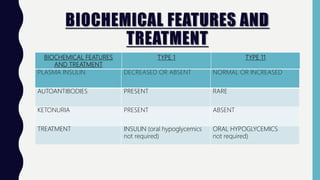
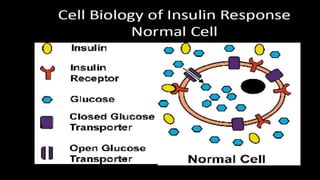
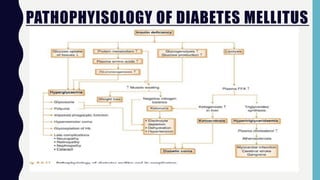
1. Diabetes mellitus is a metabolic disorder characterized by high blood glucose levels due to defects in insulin production, insulin action, or both.
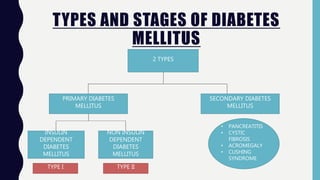
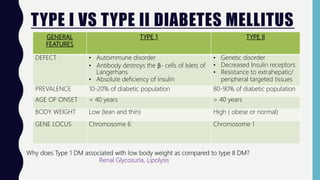
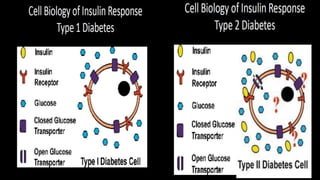
2. There are two primary types of diabetes - type 1 caused by autoimmune destruction of insulin-producing beta cells and type 2 related to insulin resistance.
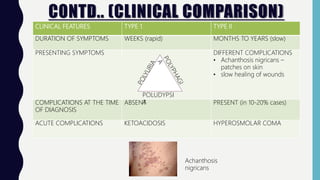
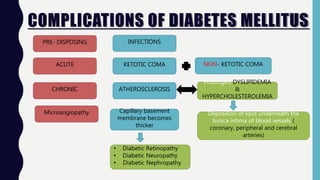
3. Uncontrolled diabetes can lead to serious complications affecting many parts of the body like the eyes, kidneys, heart, blood vessels, and nerves due to effects of long-term high blood glucose levels like glycosylation of proteins.