Download as PDF, PPTX




![• Australia has introduced the National Disability
Insurance Scheme
• All disabled people (under 65!) will get a fully
funded, non-means-tested, personal budget
• Led to most popular tax ever in a country with one
of the lowest public spending levels in developed
world.
• Similar changes now being introduced for older
people [‘Consumer Directed Care’]](https://image.slidesharecdn.com/sha-160620083131/85/Developing-a-new-policy-for-social-care-30-320.jpg)



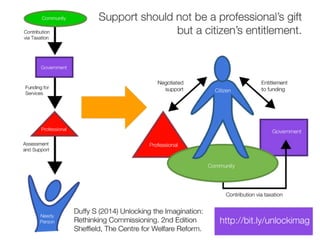
Dr. Simon Duffy discusses a new policy for social care emphasizing the importance of progressive funding and the integration of services to support people with disabilities. He criticizes the current system for being ineffective and failing to prioritize the rights and needs of disabled individuals. Recommendations include creating a human rights-based framework for social care that empowers citizens and eliminates unnecessary procurement processes.





















































































