Download as PDF, PPTX



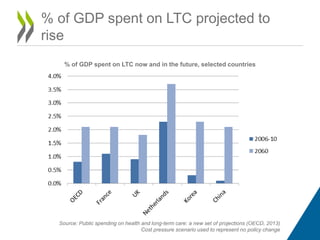
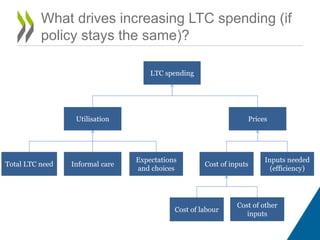
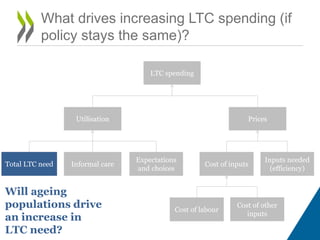
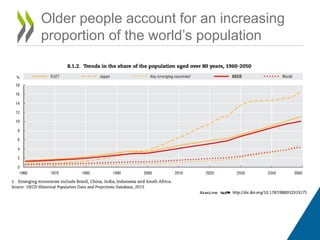
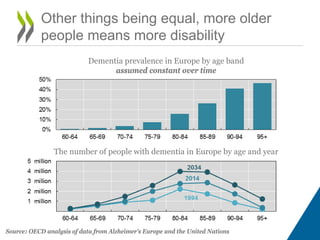

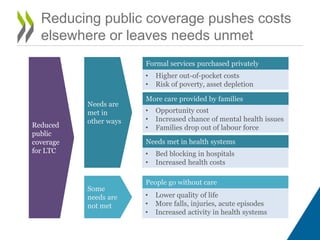
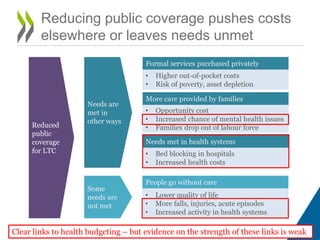
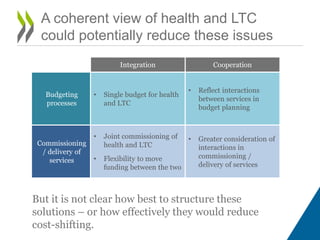

The document discusses the fiscal sustainability of long-term care (LTC) systems amid increasing costs and aging populations, highlighting the need for policy-makers to find a balance between cost, coverage, and care adequacy. It identifies key drivers of rising LTC expenditures, such as aging demographics, rising expectations for care, and informal care reliance, while also examining the implications of reducing public coverage. The document encourages discussion on how to structure budgeting processes that integrate health and LTC services to manage rising demand and associated costs effectively.


















































































