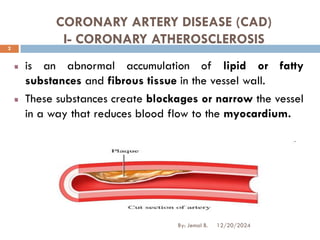
CORONARY ARTERY DISEASE(CAD)
I- CORONARY ATHEROSCLEROSIS
is an abnormal accumulation of lipid or fatty
substances and fibrous tissue in the vessel wall.
These substances create blockages or narrow the vessel
in a way that reduces blood flow to the myocardium.
12/20/2024
2
By: Jemal B.
3.
Risk Factors
Non modifiableRisk Factors
Family history of coronary
heart disease
Increasing age
Gender (heart disease
occurs three times more
often in men than in
premenopausal women)
Race (higher incidence of
heart disease in African
Americans than in
Caucasians)
Modifiable Risk Factors
High blood cholesterol and
triglyceride level
Cigarette smoking, tobacco
use
Hypertension
Diabetes mellitus
Lack of estrogen in women
Physical inactivity
Obesity
12/20/2024
3
By: Jemal B.
4.
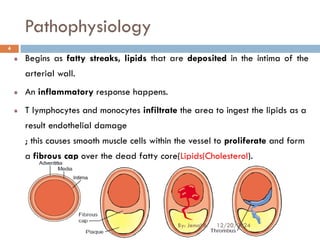
Pathophysiology
Begins as fattystreaks, lipids that are deposited in the intima of the
arterial wall.
An inflammatory response happens.
T lymphocytes and monocytes infiltrate the area to ingest the lipids as a
result endothelial damage
; this causes smooth muscle cells within the vessel to proliferate and form
a fibrous cap over the dead fatty core(Lipids(Cholesterol).
12/20/2024
4
By: Jemal B.
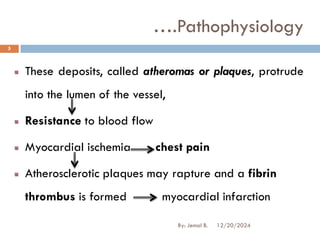
5.
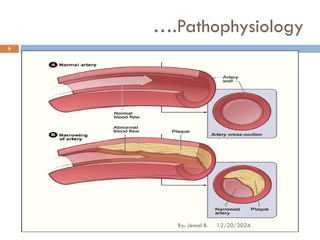
These deposits, calledatheromas or plaques, protrude
into the lumen of the vessel,
Resistance to blood flow
Myocardial ischemia chest pain
Atherosclerotic plaques may rapture and a fibrin
thrombus is formed myocardial infarction
….Pathophysiology
12/20/2024
5
By: Jemal B.
Common types ofAngina
a) Stable angina
Predictable and consistent pain of short duration,
easily relieved
Precipitated by effort or some activity (running,
walking, etc.)
Typical presentations are that of chest discomfort
b) Unstable angina "crescendo angina;“
symptoms occur more frequently and longer lasting
>10 min, more severe,
may not be relieved by rest/nitroglycerin
12/20/2024
9
By: Jemal B.
10.
c) Refractory angina
severeincapacitating pain;
Do not respond to conventional therapy including drugs
and pt may suffer severe chest pain
d) Variant angina
Pain at rest usually at night
e) Silent angina
objective evidence of ischemia (such as ECG changes),
but patient reports no symptoms
…..Common types of Angina
12/20/2024
10
By: Jemal B.
Prevention
Can be bythe control of the following four
modifiable risk factors of CAD
Increased Cholesterol
Cigarette Smoking
DM
Hypertension 12/20/2024
12
By: Jemal B.
13.
I. Controlling cholesterollevel
Desired goal is to have low LDL and high HDL
values
The desired level of LDL depends on the patient:
< 160 mg/dL for patients with one risk factors
< 130 mg/dL for patients with two or more risk factors
< 100 mg/dL for patients with CAD
HDL > 40-60 mg /dL
…..Prevention
12/20/2024
13
By: Jemal B.
14.
Non-Drug Management
Dietary measures
Weightreduction
Increased physical activity
Promoting cessation of tobacco use
Early detection and treatment of hypertension
Controlling DM 12/20/2024
14
By: Jemal B.
15.
Drug Management
Medications thatdecrease LDL, triglycerides and that
increase HDL
Niacin : Decreased blood lipids
lower LDL and triglyceride levels, and increase HDL
levels.
12/20/2024
15
By: Jemal B.
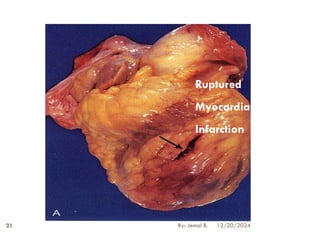
MYOCARDIAL INFARCTION
Coronary occlusion,heart attack, and MI are terms
used synonymously, but the preferred term is MI
MI refers to the process by which areas of myocardial
cells in the heart are permanently destroyed.
12/20/2024
17
By: Jemal B.
18.
Causes:
Reduced blood flowin a coronary artery
Decreased oxygen supply and
Increased demand for oxygen
.....Myocardial Infarction
12/20/2024
18
By: Jemal B.
19.
Risk Factors
Hypercholesterolemia -high LDL, low HDL
Tobacco smoking, Alcohol, OCP
Air pollution: CO,
Advanced age
Gender (men)
Diabetes mellitus, Obesity (BMI >30 kg/m²)
High blood pressure, Lack of physical activity
Family history of ischemic heart disease or MI
.....Myocardial Infarction
12/20/2024
19
By: Jemal B.
20.
Pathophysiology
Atherosclerotic plaque incoronary artery
Plaques can become unstable, rupture, and
additionally promote a thrombus that occludes the
artery
As the cells are deprived of oxygen, ischemia
develops, cellular injury occurs, and over time, the lack
of oxygen results in Ischemic cascade: death of the
heart cells near the occlusion
Infarction or cell death
.....Myocardial Infarction
12/20/2024
20
By: Jemal B.
Clinical Manifestations
Chest Pain
Occurssuddenly & not relieved by rest or nitrate
Locations: retrosternal, radiating to the neck, jaw, and arms or
to the back
May occur while the patient is active or at rest, asleep or walk
Commonly occurs in the early morning
Usually lasts for 20 minutes
Palpitations.
Heart sounds may include S3, S4, and new onset of a
murmur.
Increased jugular venous distention 12/20/2024
22
By: Jemal B.
23.
❑ Shortness ofbreath
❑ Cool, pale, and moist skin.
❑ tachycardia and tachypnea.
❑ Dysrhythmias
❑ Anxiety, restlessness, light headedness
…..Clinical Manifestations
12/20/2024
23
By: Jemal B.
24.
Dx
❑ PATIENT HISTORY:the description of the presenting
symptom (eg, chest pain) and the history of previous
illnesses and family health history, particularly of
heart disease.
❑ ECG
❑ LABORATORY TESTS: increased Creatine, increased
Myoglobin, increased Troponin
12/20/2024
24
By: Jemal B.
25.
Non-drug treatment (General
measures)
BedRest
Bowel
→ Constipation
Stool softener & Laxatives
Diet
Low fat, low Sodium , high fiber diet.
Sedation
↓Anxiety & ensures adequate sleep
Diazepam 5mg 3-4x/day , Additional dose at bed time
12/20/2024
25
By: Jemal B.
Medical Management
Drug treatment(DACA):
Oxygen, 2-4 l/min, via facemask
PLUS
Nitroglycerin, 0.5mg, sublingual, every 5 min up to 3 doses.
PLUS
Acetylsalicylic acid, 160-325 mg. P.O. QID
PLUS
Diazepam, 5mg P.O. 3-4 times daily.
PLUS
Morphine, (for control of pain), 2-4 mg IV. every 5 min until the desired
level of analgesia is achieved or until unacceptable side effects occur.
PLUS
Heparin: For all patients with myocardial infarction (MI), 7500 units
subcutaneously every 12 hours BID until the patient is ambulatory
12/20/2024
27
By: Jemal B.
28.
Followed by:
Warfarin,for at least 3 months
PLUS
Enalapril, 5 - 40 mg P.O. once or divided into two to three
doses daily
PLUS
Metoprolol, 5 mg I.V. every 2 to 5 min for a total of 3
doses
Medical Management
12/20/2024
28
By: Jemal B.
29.
HEART FAILURE
❖ HF,often referred to as congestive heart failure
(CHF), is the inability of the heart to pump sufficient
blood
❖ to meet the needs of the tissues for oxygen and nutrients.
❑ The term HF indicates myocardial heart disease
12/20/2024
29
By: Jemal B.
30.
❑ Systolic heartfailure- an alteration in ventricular
contraction.
❑ Results when the ventricle is unable to contract forcefully during
systole to eject adequate amount of blood into the circulation
❑ Diastolic heart failure- an alteration in ventricular filling
❑ Occurs when the left ventricle is unable to relax adequately during
diastole resulting in decreased ventricular filling and inadequate CO
Classification of HF
12/20/2024
30
By: Jemal B.
31.
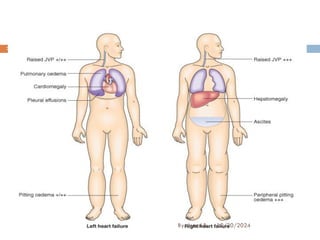
❑ Left sidedHF: - results from left ventricle dysfunction,
❑ which causes blood to back up through the left atrium and into
the pulmonary veins increasing pulmonary pressure.
❑ cause pulmonary congestion & Edema
❑ Right sided HF:- results from a diseased right ventricle (RV)
that causes back ward flow of blood to the right atrium (RA)
and venous circulation
❑ causing peripheral edema, hepatomegally, spleenomegally,
congestion of the GI tract
…..Classification of HF
12/20/2024
31
By: Jemal B.
32.
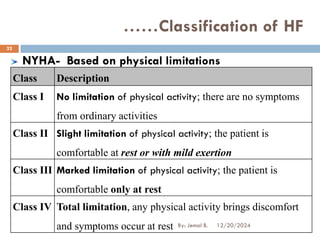
NYHA- Based onphysical limitations
Class Description
Class I No limitation of physical activity; there are no symptoms
from ordinary activities
Class II Slight limitation of physical activity; the patient is
comfortable at rest or with mild exertion
Class III Marked limitation of physical activity; the patient is
comfortable only at rest
Class IV Total limitation, any physical activity brings discomfort
and symptoms occur at rest
……Classification of HF
12/20/2024
32
By: Jemal B.
33.
Stages of CHF-The American College of Cardiology
/American Heart Association
Stage A: patients who are at high risk for developing HF but without
structural heart disease or symptoms of HF E.g., patients with DM or Hth
Stage B: patients with structural heart disease but without symptoms of
HF
Stage C: Structural heart disease and symptoms of HF
Stage D: patients requiring special interventions (end-stage
heart failure)
……Classification of HF
12/20/2024
33
By: Jemal B.
FRAMINGHAM CRITERIA FORTHE DIAGNOSIS OF
HEART FAILURE
MAJOR CRITERIA
PND or orthopnea
neck vein distention
cardiomegaly
S3/gallop
Acute pulmonary edema
12/20/2024
41
By: Jemal B.
42.
MINOR CRITERIA
Bilateral ankleedema
Night cough
Dyspnea on exertion
Hepatomegaly
Pleural effusion
Tachycardia(heart rate >120 beats/min)
The diagnosis of chronic heart failure requires the
simultaneous presence of at least 2 major criteria or 1
major criterion in conjunction with 2 minor criteria
….FRAMINGHAM CRITERIA ..
12/20/2024
42
By: Jemal B.
43.
Management
General Measures
Activity
❑Heavy physicallabor is not recommended
❑Routine modest exercise for class I–III HF
within limits of symptoms
Diet
Low sodium diet (< 2g -3g /day)
Avoid excessive fluid intake
12/20/2024
43
By: Jemal B.
44.
Main Goals OfTherapy
To eliminate or reduce etiologic or contributing
factors
To reduce the workload on the heart (preload ,
contractility & after load)
12/20/2024
44
By: Jemal B.
45.
Pharmacologic therapy
1. ACE- inhibitors (ACE-Is):
Promotes vasodilatation & diuresis by decreasing
preload & after load
Include: captopril, enalapril, lisinopril
2. Hydralazine– Decreased systemic vascular
resistance
3. Beta blockers: reduce the constant stimulation of
the sympathetic nervous system E.g. propranolol
4. Digitalis e.g. digoxin 0.125, 0.25, 0.5 mg
- slow conduction through the atrioventricular node
12/20/2024
45
By: Jemal B.
46.
5. Diuretics: increasethe rate of urine production and
the removal of excess extracellular fluid from the body
❑ Thiazides e.g. chlorothiazide, hydrochlorothiazide
❑ Loop diuretics e.g. furosemide (lasix)
❑ Potassium sparing e.g. spironolactone
❑ Combination agents e.g. spironolactone +
hydrochlorothiazide
….Pharmacologic therapy
12/20/2024
46
By: Jemal B.
47.
According to DACAof Ethiopia
First line
Digoxin 0.125-0.375 mg po daily
Plus
Furosemide , 40-240 mg, po divided in to 2-3 doses daily
Plus
Enalapril 5-40 mg po once or divided in to two dose daily
And/or
Spironolactone 25-100mg po once daily or divided into
two doses
12/20/2024
47
By: Jemal B.
48.
Nursing Intervention
1. Maintainingnormal body fluid
Evaluating degree of peripheral edema
Daily measurement of abdominal girth
Monitoring intake & out put and daily body weight
Restriction of sodium diets & fluid
Avoid diet high in fat/cholestrol
12/20/2024
48
By: Jemal B.
49.
2. Improving activitytolerance
❑ Avoid prolonged bed rest
❑ Emotional & physical support to reduce oxygen consumption
❑ Moderate physical exercise for a total of 30 min with 3-5
times per week
❑ Monitoring patient’s response to activity
3. Maintaining skin integrity
❑ Monitor signs of edema
❑ Meticulous skin care
❑ Pad bony prominences
❑ Passive ROM to extremities every 4 hours to facilitate venous
return of the fluid
❑ Turning & repositioning the patient every 2 hours
…..Nursing Intervention
12/20/2024
49
By: Jemal B.
Blood pressure isthe product of cardiac output multiplied by peripheral
resistance. Cardiac output is the product of the heart rate multiplied by the
stroke volume.
HYPERTENSION
12/20/2024
51
By: Jemal B.
52.
HYPERTENSION
is a systolicblood pressure greater than 140 mm Hg
and a diastolic pressure greater than 90 mm Hg over
a sustained period, based on the average of two or
more blood pressure measurements taken in two or
more contacts with the health care provider after an
initial screening.
12/20/2024
52
By: Jemal B.
53.
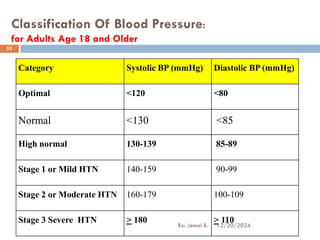
Classification Of BloodPressure:
for Adults Age 18 and Older
Category Systolic BP (mmHg) Diastolic BP (mmHg)
Optimal <120 <80
Normal <130 <85
High normal 130-139 85-89
Stage 1 or Mild HTN 140-159 90-99
Stage 2 or Moderate HTN 160-179 100-109
Stage 3 Severe HTN > 180 > 110
12/20/2024
53
By: Jemal B.
54.
Types of hypertension
1.Primary (Essential) hypertension
❖ Accounts for about 90-95% of all cases
❖ Has no known causes
❖ Onset usually between the age of 30 & 50 years
❖ factors that may contribute for the development include:
Genetic predisposition: the exact mechanism has not been established
Environment:
Dietary salt intake and Salt sensitivity
Obesity
Occupation
Family size and crowding
Stress and increased serum lipid level
Pregnancy-induced hypertension: Toxemia of pregnancy
12/20/2024
54
By: Jemal B.
55.
2. Secondary hypertension
❖In 5-10 % of patients with hypertension, the hypertension
is secondary to identifiable disorder
❖ Identifiable causes include:
Renal vascular & renal parenchymal disease
congenital abnormalities of aorta
Cushing syndrome
Brain tumors
Encephalitis
Medications
• Glucocorticoids
• Mineralocorticoids
• Sympathomimetic
12/20/2024
55
By: Jemal B.
56.
Pathophysiology
Hypertension may becaused by one or more of the
following:
❑ 1. Increased sympathetic nervous system activity
❑ 2. Increased activity of renin-angiotensin-aldosterone
system
❑ 3. Decreased vasodilation of the arterioles
❑ 4. Structural and functional changes in the heart and blood
vessels 12/20/2024
56
By: Jemal B.
57.
Clinical manifestations
Hypertension isoften called “silent killer” because it is
frequently asymptomatic especially if the hypertension
is mild or moderate.
Headache: Is the most common symptom, Occurs in the
occipital region, Worsen on the morning on arising
kidneys involvment:
Nocturia
Increased BUN & serum creatinine level12/20/2024
57
By: Jemal B.
Diagnosis
History
Physical Examination
Measuring bloodpressure (at least 1week apart)
Ophthalmologic examination
Lab tests
U/A – e.g. urine catecholamine
Blood chemistries (level of Na+, K+, Cl-, LDL etc)
Creatinine, BUN
ECG, Echocardiography & chest X-ray
12/20/2024
59
By: Jemal B.
60.
Management
The managements ofhypertension include:
Lifestyle modifications
Pharmacologic therapy
12/20/2024
60
By: Jemal B.
61.
Lifestyle Modifications
Weight reduction
Moderationof alcohol in take
Regular physical activity
Reduction of salt intake
Smoking cessation
Life style modifications are indicated for the person
with either border line or sustained hypertension
➢ If the BP remains > 140/90mmHg after 3-6 months
of life style changes, drug therapy is indicated.
….Management
12/20/2024
61
By: Jemal B.
62.
The DASH Diet
Grainsand grain products 7–8gm/day
Vegetables 4–5gm/day
Fruits 4–5gm/day
Low fat or fat-free dairy foods 2–3gm/day
Meat, fish, poultry
Nuts, seeds, and dry beans 4–5gm/weekly
12/20/2024
62
By: Jemal B.
63.
Goal-
Preventing death andcomplications by achieving
and maintaining the BP at 140/90 mmHg or lower
and
lower than 130/80 mmHg for people with DM &
chronic kidney diseases.
Pharmacologic/drug therapy
12/20/2024
63
By: Jemal B.
Calcium channel blockers:Nifidipine, Verapamil, Diltiazem
ACE I inhibitors: Captopril , Enalapril, Lisinopril
Angiotensin II receptor antagonists: Valsartan , Losartan,
Irbesartan
Diuretics: Furosemide (Lasix), Hydrochlorothiazide
….Pharmacologic
12/20/2024
65
By: Jemal B.
66.
DACA of Ethiopia
drugsused as first step agents
Diuretics
Beta Blockers
Calcium antagonists
ACE-Is
12/20/2024
66
By: Jemal B.
67.
First line drugsfor non-emergency conditions
Hydrochlorothiazide, 12.5-50 mg/day PO And/or
Nifedipine 10-40 mg, PO TID And/or
Propranolol 40-160 mg PO divided in to 2-4 doses
Alternative
Enalapril, 2.5-40 mg PO, once or divided in to two doses
daily And/or
Methyldopa, 250-2000 mg PO in divided doses. OR
Hydralazine, 10-20 mg, slow IV can be given in severe
hypertension. OR
Atenolol, 50 – 100 mg p.o daily
…..DACA of Ethiopia
12/20/2024
67
By: Jemal B.
68.
Hypertensive Crises
Blood pressureelevation to such degree can
cause vascular damage, encephalopathy, retinal
hemorrhage, renal damage and death.
1 –2% of the hypertensive population develop
this complication.
12/20/2024
68
By: Jemal B.
69.
HYPERTENSIVE EMERGENCY
❑ ishypertension with acute impairment of one or more
organ systems in which there is acute impairment of
target organ
❑ It generally occurs at the blood pressure is severely
elevated [180 or higher for systolic pressure or 120 or
higher for diastolic pressure], ,
❑ but can occur at even lower levels in patients whose blood
pressure had not been previously high
❖ In these conditions, the blood pressure should be
lowered aggressively over minutes
❑ Progressive end-organ dysfunction.
12/20/2024
69
By: Jemal B.
70.
HYPERTENSIVE EMERGENCY
❑ Thenurse may think that taking vital signs every 5
minutes check vital signs at 15 or 30 minutes intervals if
the situation is more stable.
12/20/2024
70
By: Jemal B.
71.
HYPERTENSIVE URGENCY
❑ urgencyis a situation where the blood pressure levels
exceeding 180 systolic OR 110 diastolic but there is no
associated organ damage.
❑ No progressive target-organ dysfunction
❑ Treatment of hypertensive urgency requires readjustment
and/or additional dosing of oral medications,
❑ but most often does not necessitate hospitalization for rapid
blood pressure reduction
12/20/2024
71
By: Jemal B.
72.
Clinical Manifestation
The eyes:may show retinal hemorrhage
The brain: headache, vomiting, and/or subarachnoid or
cerebral hemorrhage
shows manifestations of increased intracranial pressure
The kidneys: hematuria, proteinuria, and acute renal
failure
CVS: Patients will usually suffer from left ventricular
dysfunction
Other : Chest pain, Arrhythmias, Epistaxis, Dyspnea,
Faintness or vertigo, Severe anxiety 12/20/2024
72
By: Jemal B.
73.
Treatment of HypertensiveEmergency
❑ Hydralazine, 5 mg IV every 15-min should be given
until the mean arterial
❑ blood pressure is reduced by 25% (within minutes to 2
hours),
❑ furosemide, 40 mg IV can be used according to
blood pressure response
12/20/2024
73
By: Jemal B.
74.
Treatment of HypertensiveUrgency
❑ Nifedipine, 20-120 mg p.o in divided doses per day
could be used. OR
❑ Captopril, 25-50 mg p.o three times daily
12/20/2024
74
By: Jemal B.
75.
Nursing Interventions
❑ Improvingactivity tolerance
❑ Alleviating pain:
❑ encourage/maintain bedrest during acute phase.
provide/recommend nonpharmacological measures
❑ Patient education about lifestyle modifications
❑ Compliance to therapeutic regimens
❑ Nutritional advice
❑ Avoiding potential complication
12/20/2024
75
By: Jemal B.
ANEMIA
Anemia is aqualitative or quantitative deficiency of
hemoglobin, in red blood cells that transports oxygen.
It is a lower-than-normal number of red blood cells, usually
measured by a decrease in the amount of hemoglobin.
Is the most common disorder of blood which leads to hypoxia
in organs.
Not specific disease but a sign of underlying disorder.
12/20/2024
By: Jemal B.
77
78.
Potential causes
1. Lossof RBCs—bleeding, (eg. GIT, uterus, nose, or wound)
2. Decreased production of RBCs (ineffective
erythropoiesis):.
3. Hemolysis: overactive spleen (e.g. hypersplenism) or
production of abnormal RBCs (eg, sickle cell anemia)
12/20/2024
By: Jemal B.
78
79.
Specific Types OfAnemia
1. Vitamin B12/ Cobalamin Deficiency Anemia
Also called Pernicious anemia
Vitamin B12 is essential for normal nervous system function
and blood cell production.
For vitamin B12 to be absorbed by the body, it must bind to
intrinsic factor, a protein secreted by cells in the stomach.
➢ Source: Dairy products, eggs, fish, meat, and poultry
79
12/20/2024
By: Jemal B.
80.
Causes
Diet low invit B12 (e.g. strict vegetarian)
Chronic alcoholism
Abdominal or intestinal surgery
Intestinal malabsorption disorders
Tape worm
12/20/2024
By: Jemal B.
80
81.
2. Folate-deficiency Anemia
Referredto as megaloblastic anemia
Folate, also called folic acid, is necessary for RBC formation
and growth.
Folate is not stored in the body in large amounts,
Occurs in about 4 out of 100,000 people.
➢ Source: Green leafy vegetables and liver.
81
12/20/2024
By: Jemal B.
82.
Cause/Risk factors
Poor dietaryintake of folic acid
Eating overcooked food
Malabsorption diseases
Certain medications e.g. phenytoin
Third trimester of pregnancy
Alcoholism
12/20/2024
By: Jemal B.
82
83.
3. Iron DeficiencyAnemia
it is the most common form of anemia
Decrease number of RBC in blood result too little
iron.
RBCs are not providing adequate oxygen to body
tissues.
Source: meat (liver), fish and poultry
12/20/2024
By: Jemal B.
83
84.
Causes
Too little ironin the diet
Poor absorption of iron by the body
Loss of blood (including from heavy menstrual bleeding)
Risky groups
♣ Women of child-bearing age
♣ Pregnant or lactating women
♣ Infants, children, and adolescents in rapid growth
♣ People with a poor dietary intake of iron
♣ Blood loss: peptic ulcer, long term ASA use, colon ca
84
12/20/2024
By: Jemal B.
85.
4. Hemolytic Anemia
Inadequatenumber of circulating RBCs caused by
hemolysis greater than erythropoiesis.
The bone marrow is unable to compensate for premature
destruction.
85
12/20/2024
By: Jemal B.
5. Idiopathic/Aplastic Anemia
Alsocalled pancytopenia
Is a failure of the bone marrow to properly form all
types of blood cells
Results from injury to the stem cell
Cause is unknown, but is thought to be an
autoimmune process.
12/20/2024
By: Jemal B.
88
89.
Common Clinical ManifestationOf Anemia
Paleness
Yellow eyes/skin
Fatigue
Breathlessness
Rapid heart rate
Delayed growth and puberty
12/20/2024
By: Jemal B.
89
▪Susceptibility to infections
▪Ulcers on the lower legs
▪Jaundice
▪Bone pain
▪Fever
90.
Assessment and DiagnosticFindings
Physical Exam & history
CBC
Hgb concentration, Hct,
ESR, folate level, serum vit B12
Iron tests (serum level, binding capacity, % saturation)
Bone marrow aspiration and biopsy
Elevated bilirubin
Erythropoietin levels
12/20/2024
By: Jemal B.
90
91.
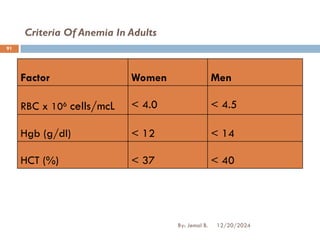
Criteria Of AnemiaIn Adults
12/20/2024
By: Jemal B.
91
Factor Women Men
RBC x 106 cells/mcL < 4.0 < 4.5
Hgb (g/dl) < 12 < 14
HCT (%) < 37 < 40
92.
Treatments For Anemia
Treatmentdepends on severity and the cause.
Treatment goals:
➢To get RBC counts or Hgb levels back to normal
➢To treat the underlying cause of the anemia
12/20/2024
By: Jemal B.
92
93.
Iron deficiency anemia
Ironsupplements- for several months or longer
If the underlying cause of iron deficiency is loss of blood,
the source of bleeding must be located and stopped.
Food rich in iron: Meat, poultry, fish, eggs, dairy products, or
iron-fortified foods.
Ferrous sulfate :300mg PO TID for 4-6 months
Prophylactic therapy: pregnancy, sever hemolytic anemia,
in patients with dialysis
12/20/2024
By: Jemal B.
93
94.
Management …
Vit B12Deficiency: is treated with which is given parentraly
Initial dose: 30 mcg IM daily for 5 to 10 days Maintenance dose: 100 to
200 mcg IM monthly.
Prophylactic therapy is indicated in patients with Total
gastrectomy and Ileal resection
Folate deficiency
Dose: Folic acid 5 mg Po daily
Prophylactic therapy is indicated in pregnancy, sever hemolytic
anemia, in patients with dialysis, and premature newborns
94
12/20/2024
By: Jemal B.
95.
Anemia Of ChronicDisease
It can be focused on treating the underlying disease.
Iron and vitamin supplements don't help
If symptoms become severe, a blood transfusion or
injections of synthetic erythropoietin, may help stimulate
RBC production.
12/20/2024
By: Jemal B.
95
96.
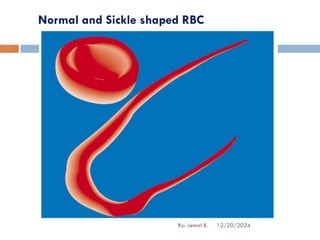
Sickle Cell Anemia
Rx for this incurable anemia include:
♣Cancer drug hydroxyurea (Droxia)
♣A bone marrow transplant
♣Blood transfusions
➢Supportive:
♣Administration of oxygen
♣Pain-relieving drugs
♣Oral and intravenous fluids
96
12/20/2024
By: Jemal B.
97.
Prevention Of Anemia
➢Eat foods high in iron
➢ Make sure to consume enough folic acid and vit. B12
➢ “Don't drink coffee or tea with meals”.
➢ Talk to doctor about taking iron pills (supplements):
ferrous and ferric.
12/20/2024
By: Jemal B.
97


![HYPERTENSIVE EMERGENCY
❑ is hypertension with acute impairment of one or more
organ systems in which there is acute impairment of
target organ
❑ It generally occurs at the blood pressure is severely
elevated [180 or higher for systolic pressure or 120 or
higher for diastolic pressure], ,
❑ but can occur at even lower levels in patients whose blood
pressure had not been previously high
❖ In these conditions, the blood pressure should be
lowered aggressively over minutes
❑ Progressive end-organ dysfunction.
12/20/2024
69
By: Jemal B.](https://image.slidesharecdn.com/cvdformidwifery-250302222215-d26c6138/85/CVD-for-midwifery-pdf-for-the-second-year-69-320.jpg)