Cutaneous Reaction
To PhysicalAgents
Dr . Hindreen Aqrawi
Dermatologist at Azadi teaching general hospital
Duhok – KRG/ Iraq
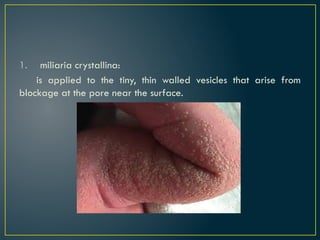
2.
Reaction to cold
Reactionto abnormal cold exposure :
May occur in any individual over exposed to excessive cold.
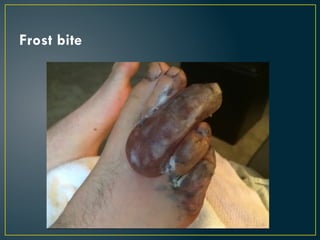
Example : frost bite
It started as painful erythema, swelling or even blister….. If
persist gangrene and even spontaneous amputation
of the affected parts .
o Abnormal reactionto usual cold exposure :
Occurs only in small susceptible proportion of the population.
probably genetically predispose.
Example: chilblain, cryoglobullinemia and others.
6.
Perniosis ( chilblains)
oAn abnormal vascular response to cold exposure.
o Chilblains are painful, inflammatory lesions provoked by
exposure to cold.
o They particularly affect older children and young adults.
o The lesions occur on the fingers, toes and occasionally elsewhere.
o It presented as raised, dusky red swellings.
o are painful and/or itchy.
Reaction to theheat
1- Erythema ab igne:
It is occurs in patients exposed frequently to Infra red radiation
from heat sources for long time. causes injury to the skin.
It presented as brownish-red reticulate pigmentation.
keratoses and even squamous cell carcinoma can also occur at
involved sites.
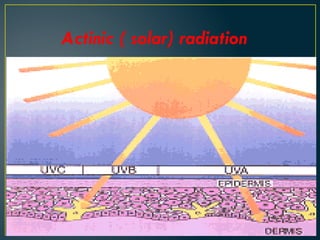
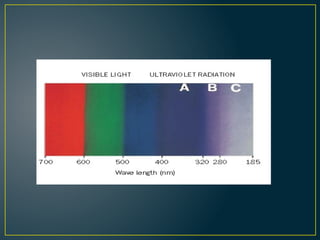
The sunemits a continuous band of energy over a
wide range of wavelengths, but it is only the UVR
(200–400 nm) that is of major importance .
Three segments of UVR are recognized:
UVC
200–290 nm.
mostlyfiltered out by the ozone layer.
only become biologically important if the ozone layer became
seriously depleted.
22.
Normal Reactions toExcessive Sun Exposure
1. Acute effects:
A. Skin pigmentation: Immediate pigment darkening and
delayed tanning.
B. Sun burn.
23.
2. Chronic effects:
A.photo aging of the skin:
Excessive wrinkling.
Skin atrophy
Solar lentigines.
Solar elastosis. -
Senile comedones.
Colloid millium.
Telengiectasia.
Poikiloderma of Civatte.
B. premalignant and malignant skin conditions:
These are caused mainly by UVB, ex. actinic keratosis, basal cell carcinoma, squamous cell
carcinoma and malignant melanoma.
24.
Abnormal Reactions toSun Exposure(Photodermatoses)
I. Metabolic diseases: ex. Porphyria, xerodenna pigmentosum,
pellagra.
2. Drug induced (topical and systemic drugs).
3. Diseases aggravated by sunlight:
- Actinic lichen planus
-Erythema multiforme
-Lupus erythematosus
-Vitiligo
-Psoriasis
25.
4. Idiopathic photodermatosis:
Polymorphiclight eruption
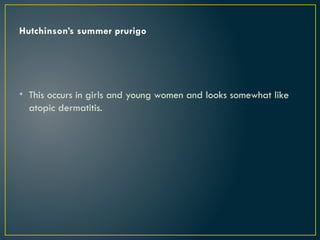
Hydroa aestivale (summer prurigo of Hutchinson)
Hydroa vacciniform
Solar urticaria
Juvenile spring eruption
Actinic reticuloid
Chronic actinic dermatitis
26.
Pigmentation
Immediate pigment darkening:
thisis started few minutes and last for few, hours after sun
exposure.
It is caused by photo-oxidation and darkening of the preexisting
melanin without new melanin formation.
Delayed tanning:
This is usually started few hours after sun exposure and peak in
72 hours and last for 2-4 weeks. It is caused by UVB leading to
hypertrophy and hyperplasia of melanocytes and new melanin
formation.
27.
Sunburn
This isa very common condition that occurs when the patient
exposed to excessive sunlight. It is mainly caused by UVB and rarely
by UVA.
It usually starts few hours after sun exposure as erythema
associated with burning sensation, oedema and swelling. Vesicles and
bullae may occur in severe conditions.
Severe systemic symptoms may occcur.
Treatment:
cold bath and cold dressing topical steroids
antihistamines
Antiprostaglandins: indomethacin or aspirin orally.
28.
Photosensitivity reactions
Skincan become sensitized to a specific part of the solar
spectrum by chemical agents that reach it either via the systemic
route or after contacting the skin topically.
29.
Photosensitivity consists oftwo types:
Phototoxicity: this can occur in any patient when exposed even
for the first time to sufficient dose of the offending drug that is
followed by sun exposure. The patient develops sunburn like
picture clinically.
30.
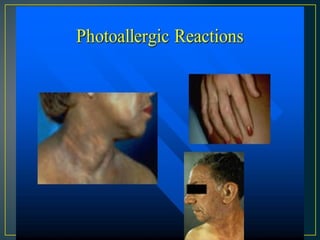
Photoallergic reaction: occursonly in
predisposed individuals and needs previous
exposure and sensitization. It appear clinically
as dermatitis like reaction on re-exposure even
to small dose of the drug i.e. dose independent.
32.
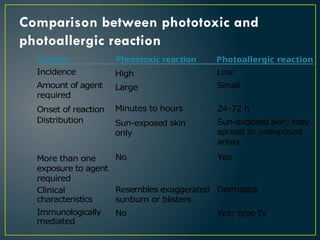
Comparison between phototoxicand
photoallergic reaction
Feature Phototoxic reaction Photoallergic reaction
Incidence
Amount of agent
required
Onset of reaction
Distribution
High
Large
Minutes to hours
Sun-exposed skin
only
Low
Small
24-72 h
Sun-exposed skin; may
spread to unexposed
areas
More than one
exposure to agent
required
Clinical
characteristics
Immunologically
mediated
No Yes
Resembles exaggerated Dermatitis
sunburn or blisters
No Yes; type IV
33.
Some common photosensitizingagents are
• Tetracyclines
• Phenothiazines
• Amiodarone
• Nalidixic acid
Phytochemical reactions are photosensitivity responses that result
from contact with plants or their products on areas exposed to
the sun.
Example : psoralens are found in some fruits, such as the
bergamot
34.
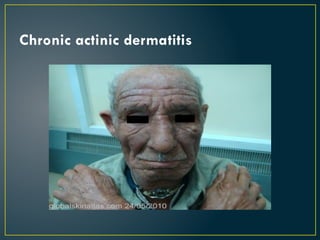
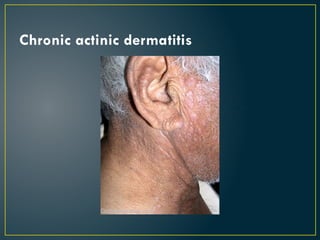
Chronic actinic dermatitis
oPatients with this disorder start with severe photoallergic
dermatitis and do not respond to routine light avoidance.
o may be markedly thickened and may be involved on all sites –
not only light exposed areas.
o The condition is then known as actinic reticuloid.
o Severely affected patients need to be nursed in a darkened
room to ensure complete protection from irradiation.
35.
They are usuallymiddle-aged or elderly men.
Exact cause is unknown But some believe minute amounts of the
drug persist in the skin indefinitely.
These patients may be exquisitely sensitive to
UVR who react after the slightest exposure.
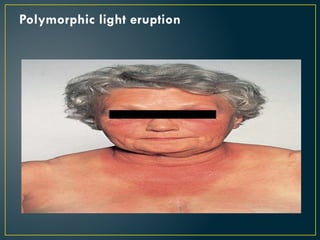
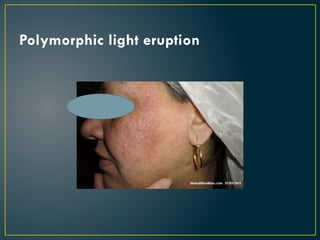
Polymorphic light eruption
The commonest light induced skin disease.
The initial symptoms include burning, itching and erythema, on
sun exposed areas (face, V area of chest, back of hands,
extensors of forearms), usually hours after sun exposure
throughout the spring and summer months, and persists for
several days.
The disease may begin at any age. Lesions usually heal without
scarring. Light sensitivity may decrease with repeated sun
exposure, a condition referred to "hardening".
39.
There are severalmorphological types:
- Papular type (the commonest form)
- Papulovesicular type
- Plaque type
- Erythema multiforme type
- hemorrhagic type
Photopatch tests
Suspectedphotosensitizers are placed on the skin and
irradiated with broad-spectrum UVR. Controls are run with
irradiation alone and with the suspected substances without
irradiation. Patches are examined for signs of eczema up to 72
hours after irradiation.
Treatment of photodermatosis
Preventionby avoidance of sun exposure and protection of the skin by
sunscreens.
Systemic sunscreens may be useful in certain conditions like chloroquine
which also have anti-inflammatory effect.
Anti-inflammatory topical steroids or even systemic steroids in sever cases.
Immunosuppressant drugs like azathioprine or cyclosporine in resistant
cases.
Therapy with sunlight sometimes used by exposing the patent to gradually
increasing doses of UVB light or by using systemic PUVA in late winter to
produce accommodation of the skin to sun exposure in spring and summer
and prevent appearance of photosensitive skin diseases. This process is
called hardening of the skin.

















































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)

![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)







