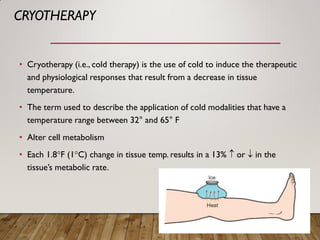
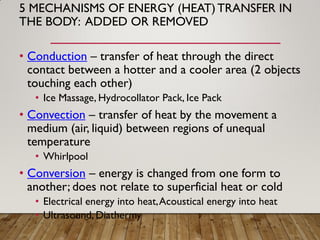
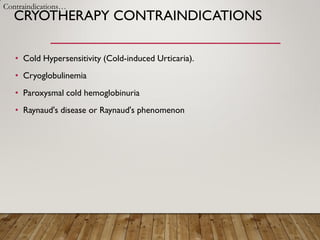
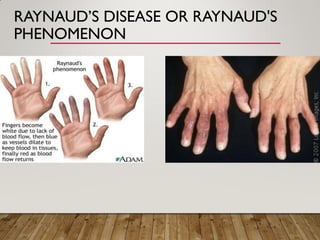
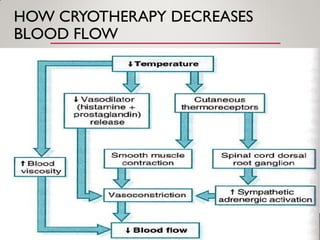
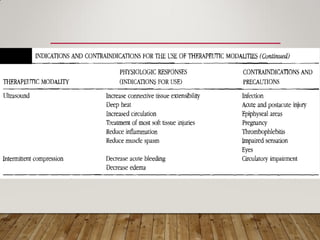
Cryotherapy involves the application of cold to induce therapeutic effects by decreasing tissue temperature. It works through mechanisms like conduction, convection, and evaporation to remove heat from the body. While cryotherapy can provide benefits like reduced pain and inflammation, it may exacerbate conditions involving impaired circulation or nerve function and cause issues in sensitive individuals. Precautions should be taken when applying cryotherapy to avoid potential contraindications or side effects.























































![Hypothalamus short notes on location, function and disorders by Dr. Neha [PT]...](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124142231-2b48143d-thumbnail.jpg?width=640&height=640&fit=bounds)




![Cells and Organs of immune system [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/cellsandorgansofimmunesystemautosaved-260123152717-ea0cb261-thumbnail.jpg?width=640&height=640&fit=bounds)










