Download to read offline



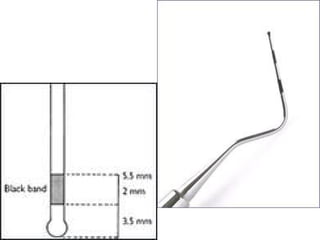
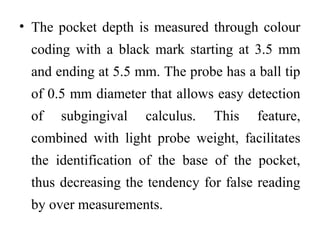


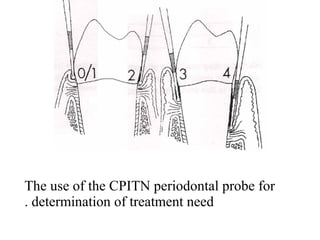

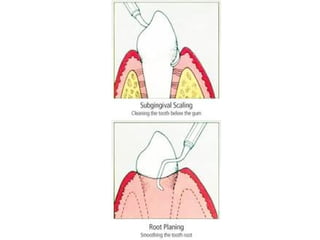
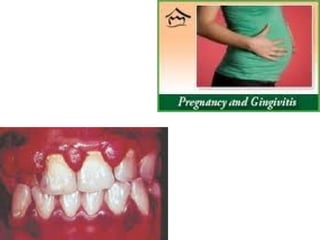
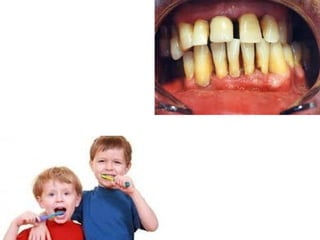











This document discusses two indices used to assess periodontal diseases: the Community Periodontal Index of Treatment Need (CPITN) and factors that affect the incidence and prevalence of periodontal diseases. The CPITN is designed to assess treatment needs in a population by recording conditions like pockets, bleeding, and calculus. It divides the mouth into sections and codes the highest need in each section. Factors that influence periodontal diseases include age, sex, oral hygiene, socioeconomic status, tobacco use, general health, nutrition, occlusion, and race. Periodontal disease severity increases with age.








































































![Hypothalamus short ppt by Dr. Neha [PT].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/hypothalamusbydr-260124145759-b9f94a93-thumbnail.jpg?width=640&height=640&fit=bounds)












