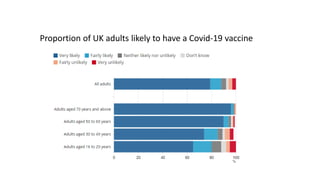
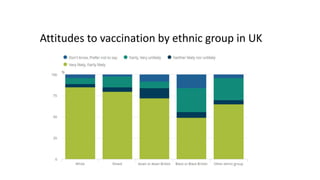
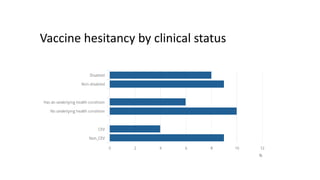
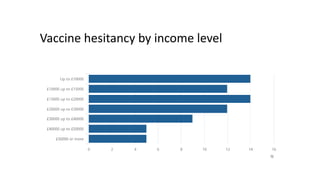
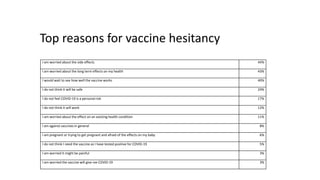
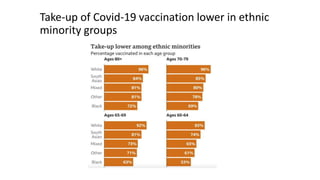
Vaccine hesitancy, defined as a delay in acceptance or refusal of safe vaccines, is recognized by WHO as a major global health threat, particularly regarding COVID-19 vaccination. Factors contributing to vaccine hesitancy include concerns about safety, effectiveness, and personal health risks, with disparities observed among ethnic groups and socioeconomic statuses. Addressing hesitancy requires tailored communication, community engagement, and systemic health interventions, emphasizing the need for trust and knowledge in promoting vaccine uptake.































![Vaccine Hesitancy[1] MBBS ABroad study.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/vaccinehesitancy1-250627110710-6d4da11b-thumbnail.jpg?width=640&height=640&fit=bounds)












































