
Download as PDF, PPTX





![European Food Safety Authority (EFSA)
•
Zucconiet al., 2013. “Gathering consumption data on specific consumer groups of energy drinks.” [190 pages] www.efsa.europa.eu/publications
•
EFSA opinion on caffeine’s safety was requested by the EC (Feb 2013); established a Working Group on Caffeine…
•
Maximum levels of caffeine intake from all sources
•
Risk of interaction of caffeine with alcohol and other ingredients of “Energy Drinks”
•
Focus: general population, adults performing physical activities of various intensities, pregnant & lactating women, children & adolescents
•
Several meetings of the Scientific Panel on Dietetic Products, Nutrition and Allergies (NDA Panel)
•
Draft Opinion will issue early November,public consultation for 6-8 weeks, adoption by Spring 2015. 45](https://image.slidesharecdn.com/coughlincaffeineasicsept92014-140912093946-phpapp01/85/Coughlin_Caffeine-Safety-at-25th-ASIC-Armenia-Colombia-Sept-9-2014-45-320.jpg)
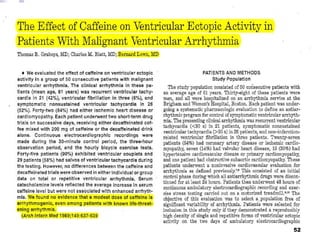
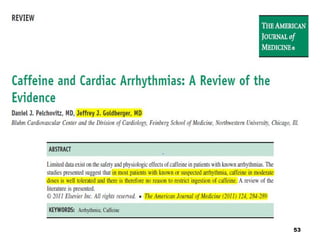

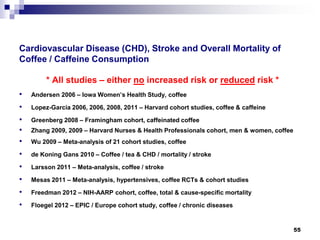
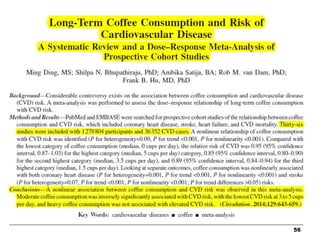

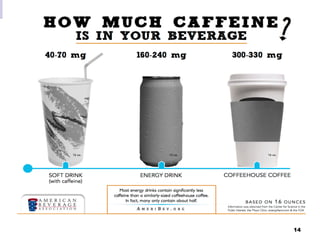
This document summarizes a presentation given on caffeine safety over three decades. It discusses how caffeine was initially linked to many health issues in animal and early human studies from the 1970s-1990s, but more recent and rigorous studies have found these links to be unsupported. It reviews topics like reproductive effects, addiction potential, bone health, cancer risk, and cardiovascular effects, finding that for typical intake levels, caffeine is generally recognized as safe. While some regulatory agencies still have concerns about new products with added caffeine, the document argues the evidence shows caffeine as consumed from coffee, tea, and soda does not pose health risks and may even provide benefits.










![Lw%20 Opportunity Mar2010[1]](https://cdn.slidesharecdn.com/ss_thumbnails/lw20opportunitymar20101-100427114044-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)



























![Coffee edited041001[1]](https://cdn.slidesharecdn.com/ss_thumbnails/coffeeedited0410011-100526143002-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)























