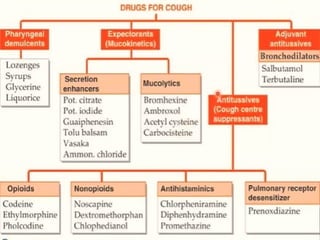
Cough is a protective reflex to clear irritants from the respiratory system, categorized into productive (helpful) and non-productive (harmful). Treatment options include expectorants, mucolytics, and antitussives, each serving different roles; expectorants facilitate mucus clearance, while antitussives suppress cough based on the type. Medications like codeine and dextromethorphan are highlighted for their antitussive properties, with various side effects and considerations for specific patient populations.