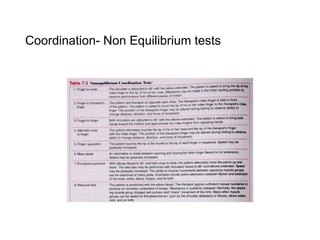
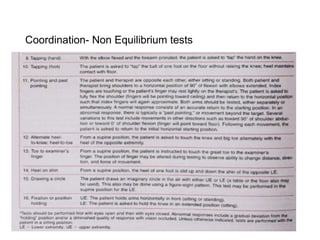
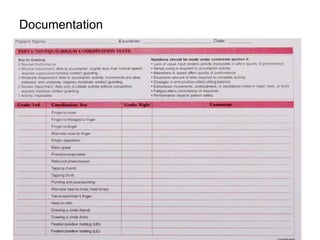
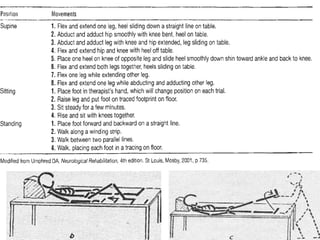
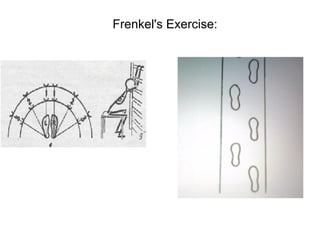
The document provides an overview of coordination in terms of muscle functioning and movement management, defining coordination as the smooth and accurate execution of motor responses influenced by various factors. It highlights causes of incoordination, such as muscle weakness or cerebellar lesions, and discusses assessment methods and reeducation principles, including Frenkel's exercises aimed at improving coordinated movement. The exercises emphasize attention, precision, and repetition to aid individuals with coordination deficits in achieving independence in daily activities.