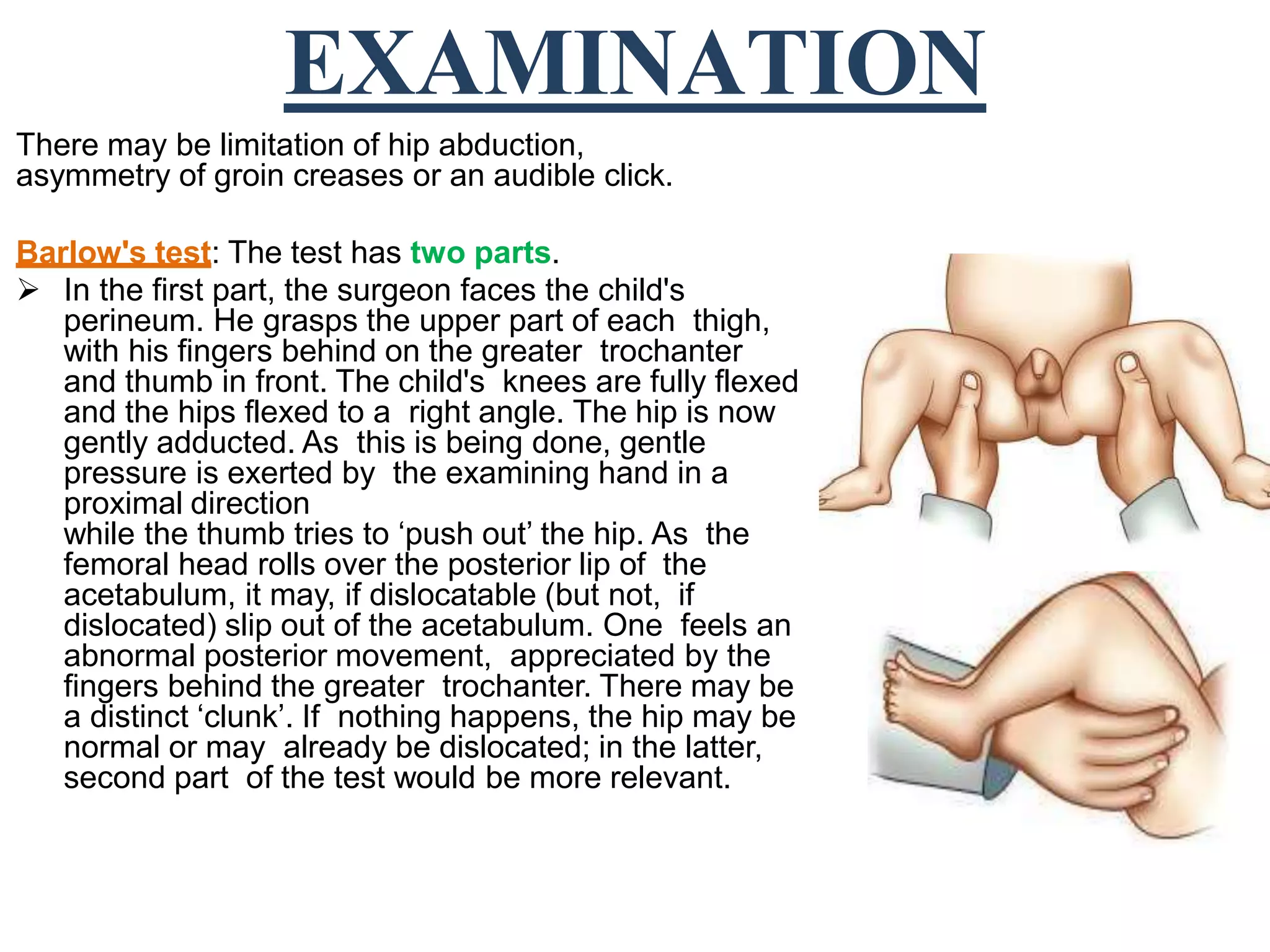
Clubfoot, congenital hip dislocation, and torticollis are congenital deformities that affect bones, muscles, tendons, and other tissues. Congenital hip dislocation occurs when the femoral head spontaneously dislocates from the acetabulum before, during, or after birth. It is diagnosed through tests like Barlow's test and Ortolani's test. Treatment aims to reduce the femoral head into the acetabulum through closed or open manipulation and maintain the reduction with casting or splinting. The treatment approach depends on the age at presentation and whether it is unilateral or bilateral.