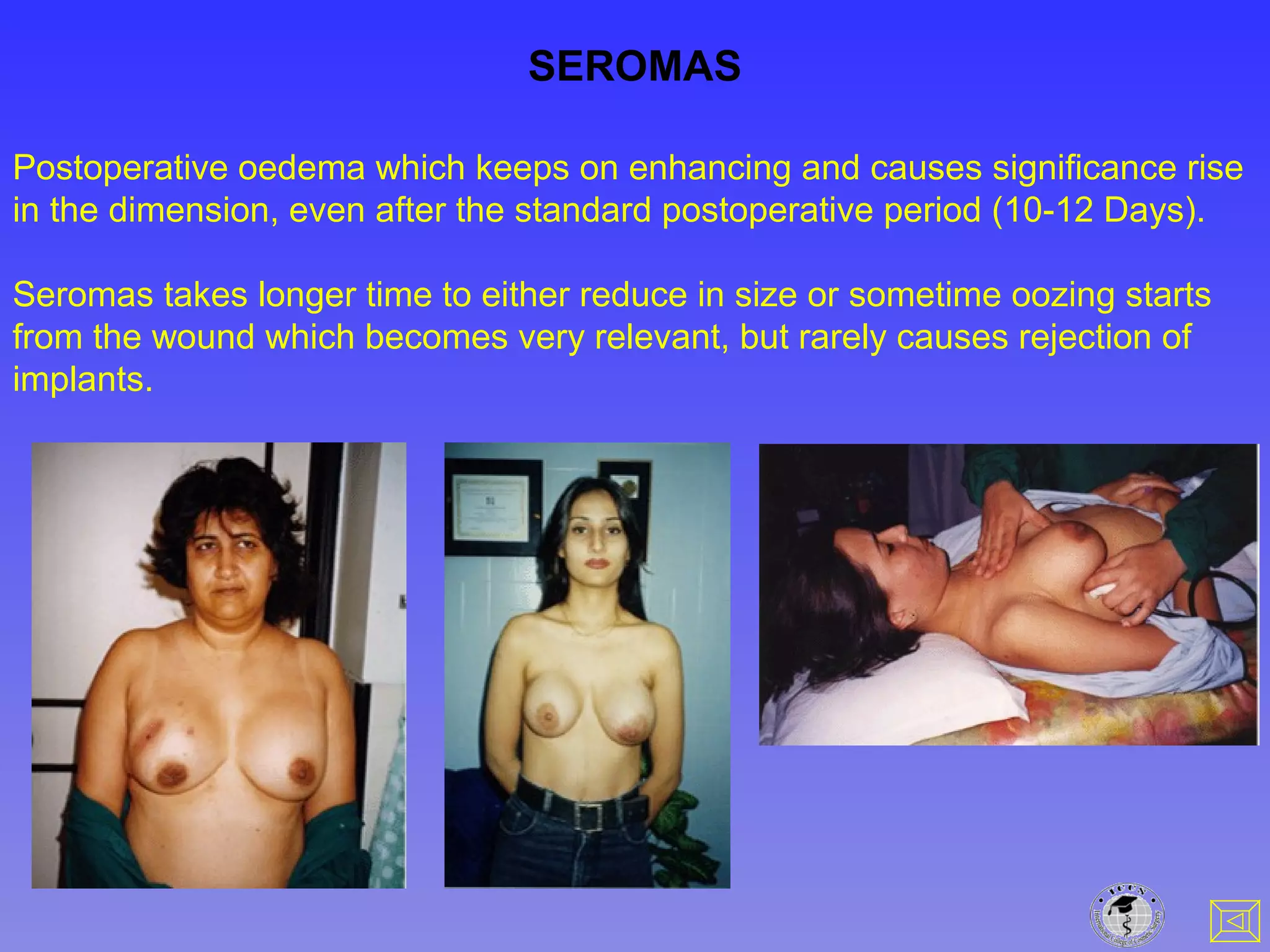
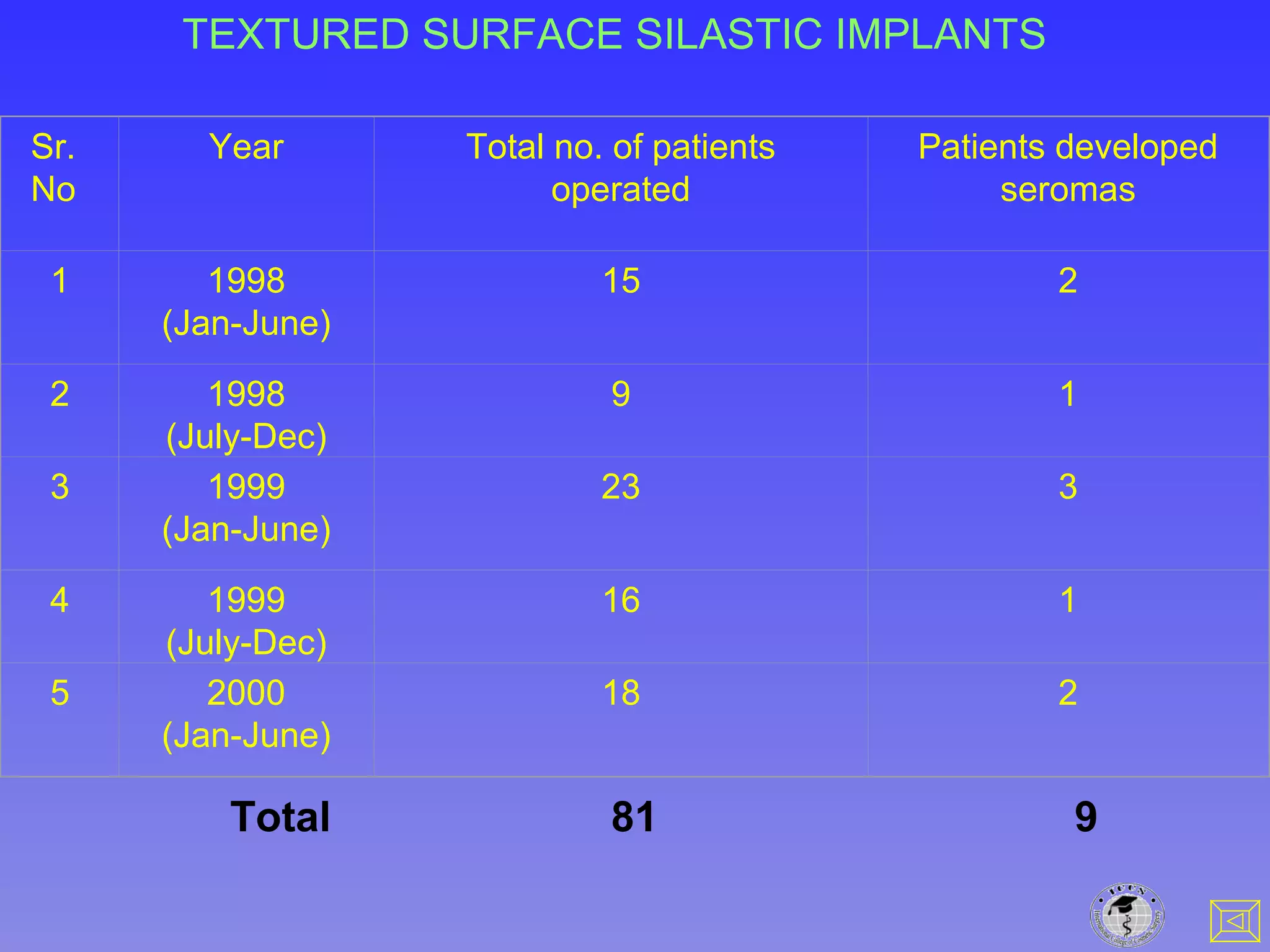
Silicone breast implants are generally considered biologically inert. However, some patients develop seromas following implantation. This document discusses several hypothesized pathophysiological pathways by which textured silicone breast implants could potentially cause generalized symptoms, but finds each of them implausible based on the scientific evidence. Specifically, silicone is unlikely to act as an antigen, adjuvant, or hapten due to its small size and inability to repeatedly bind to host molecules. A foreign body reaction and resultant cytokine production also would not be expected to cause systemic disease. The document concludes it is very unlikely that silicone breast implants can induce generalized symptoms or disease.