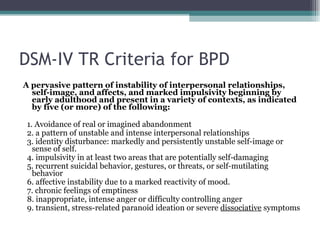
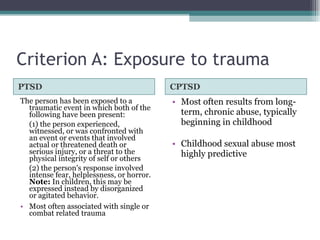
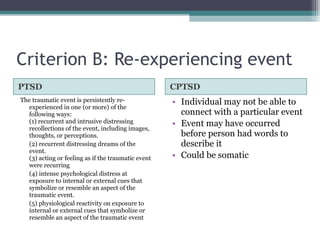
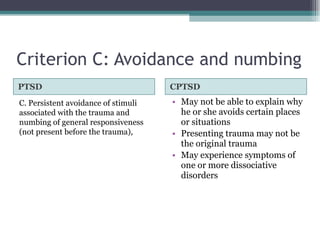
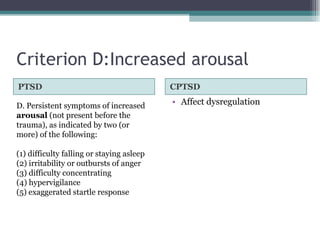
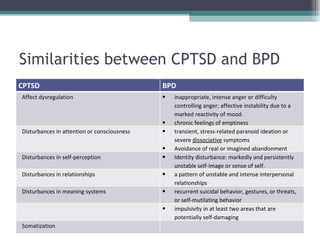
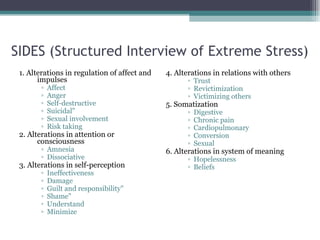
The document provides an overview and comparison of PTSD, Complex PTSD (CPTSD), and Borderline Personality Disorder (BPD). It discusses the core concepts and diagnostic criteria for each disorder. CPTSD is described as resulting from prolonged, repetitive trauma such as childhood abuse and having additional symptoms beyond classic PTSD, including affect dysregulation, consciousness/attention problems, self-perception issues, difficulties with relationships and making meaning of the world. The document notes similarities between CPTSD and BPD in several symptom domains.
![References American Psychiatric Association (2000). Diagnostic and statistical manual of mental disorders : Dsm-iv-tr (4th ed.). Washington, DC: American Psychiatric Association. Blaz-Kapusta, B. (2008). Disorders of extreme stress not otherwise specified (DESNOS) -- a case study. Archives of Psychiatry & Psychotherapy, 10(2), 5-11. Brand, B., Classen, C., Lanins, R., Loewenstein, R., McNary, S., Pain, C., et al. (2009). A naturalistic study of dissociative identity disorder and dissociative disorder not otherwise specified patients treated by community clinicians. Psychological Trauma: Theory, Research, Practice, and Policy, 1(2), 153-171. Choi, H., Klein, C., Shin, M.-S., & Lee, H.-J. (2009). Posttraumatic stress disorder (ptsd) and disorders of extreme stress (desnos) symptoms following prostitution and childhood abuse. Violence Against Women, 15(8), 933-951 Fauman, M. A. (2002). Study guide to dsm-iv-tr. Washington, DC: American Psychiatric Pub. Ford, J. D., & Smith, S. F. (2008). Complex posttraumatic stress disorder in trauma-exposed adults receiving public sector outpatient substance abuse disorder treatment. Addiction Research & Theory, 16(2), 193-203. Golier, J. A., Yehuda, R., Bierer, L. M., Mitropoulou, V., New, A. S., Schmeidler, J., et al. (2003). The relationship of borderline personality disorder to posttraumatic stress disorder and traumatic events. Am J Psychiatry, 160(11), 2018-2024. Herman, J. L. (1992). Trauma and recovery. [New York, N.Y.]: BasicBooks.](https://image.slidesharecdn.com/cptsdandbpdfinal-13204279482396-phpapp01-111104123330-phpapp01/85/Complex-PTSD-and-Bordeline-Personality-Disorder-45-320.jpg)