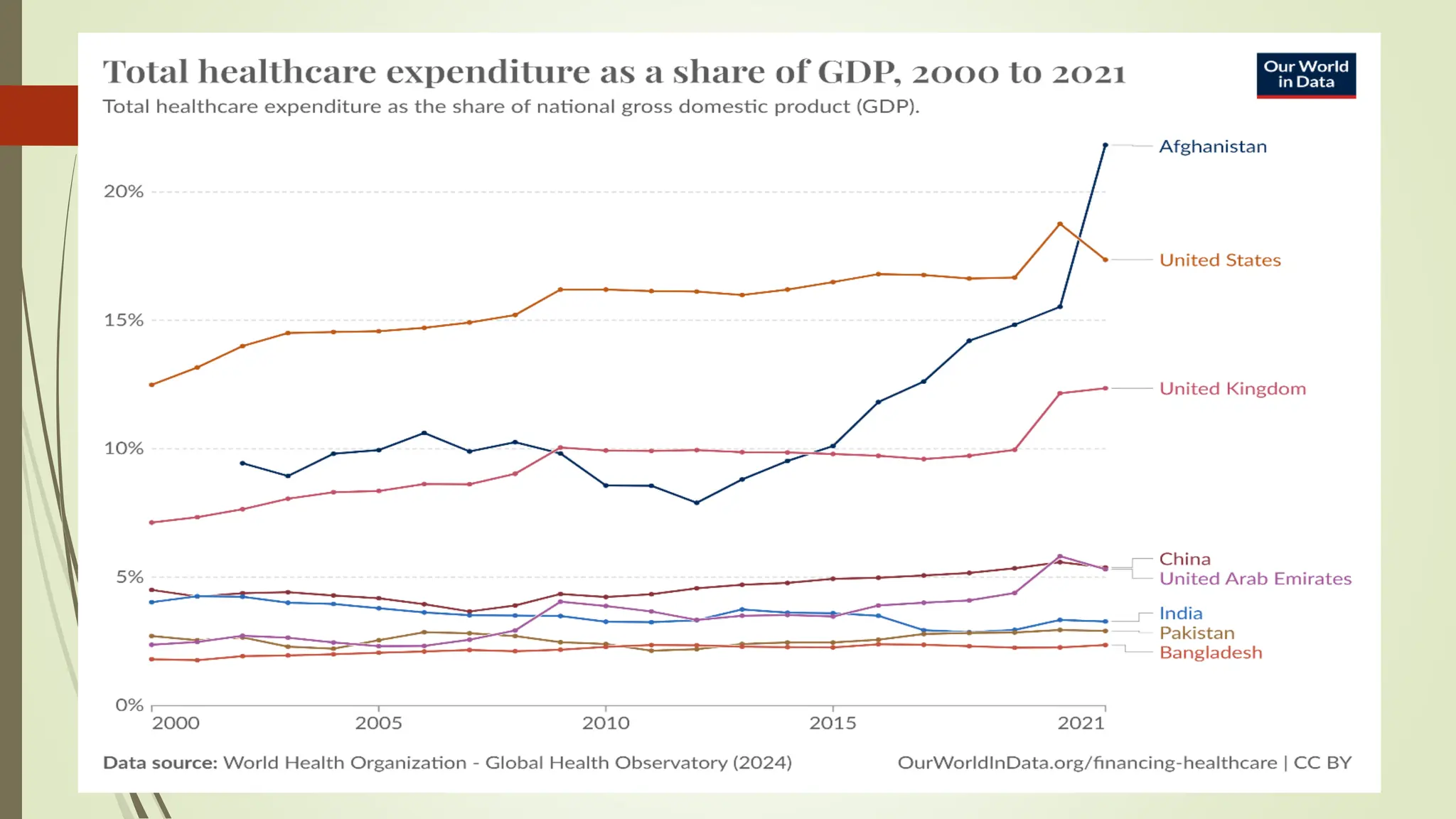
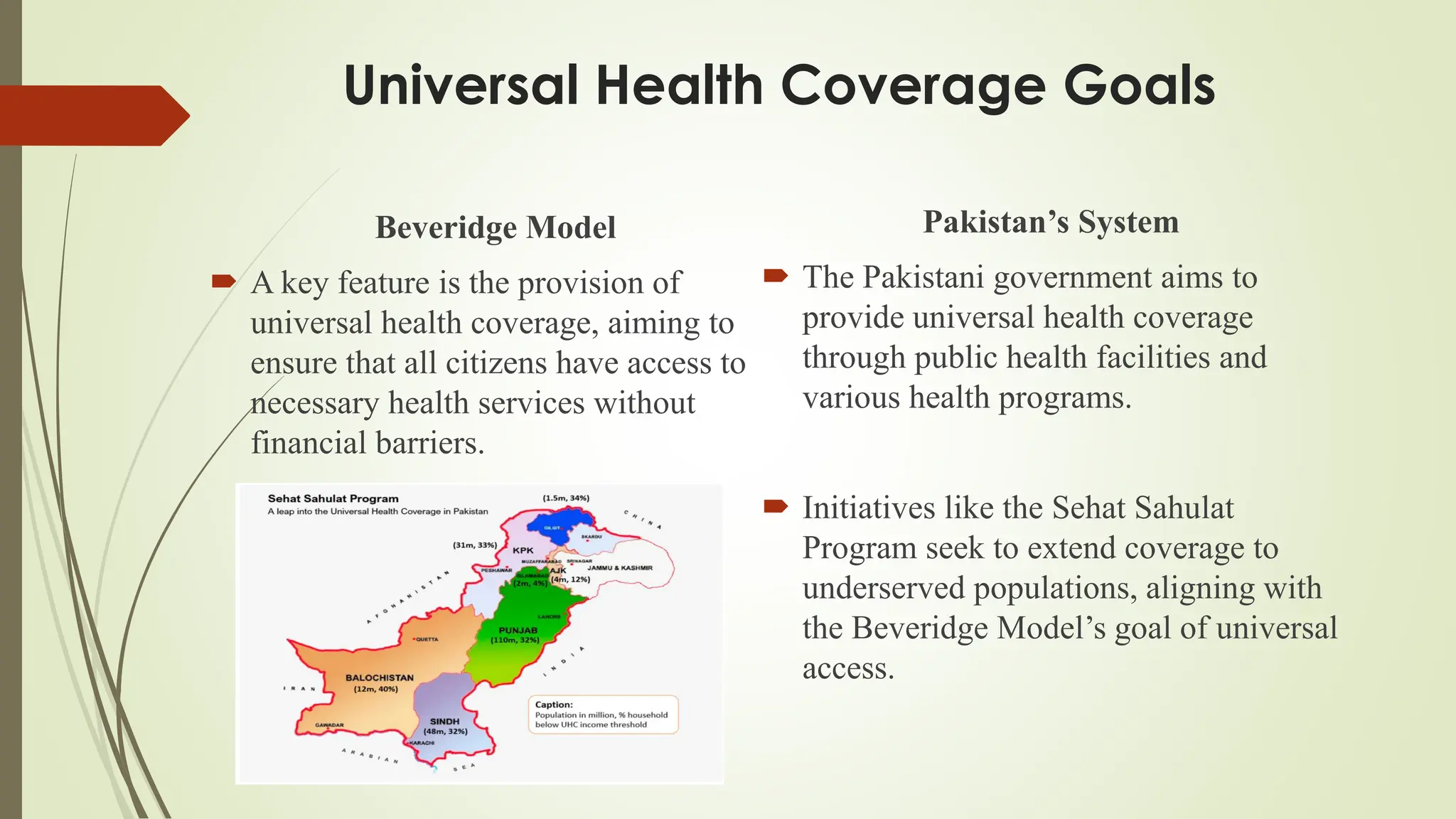
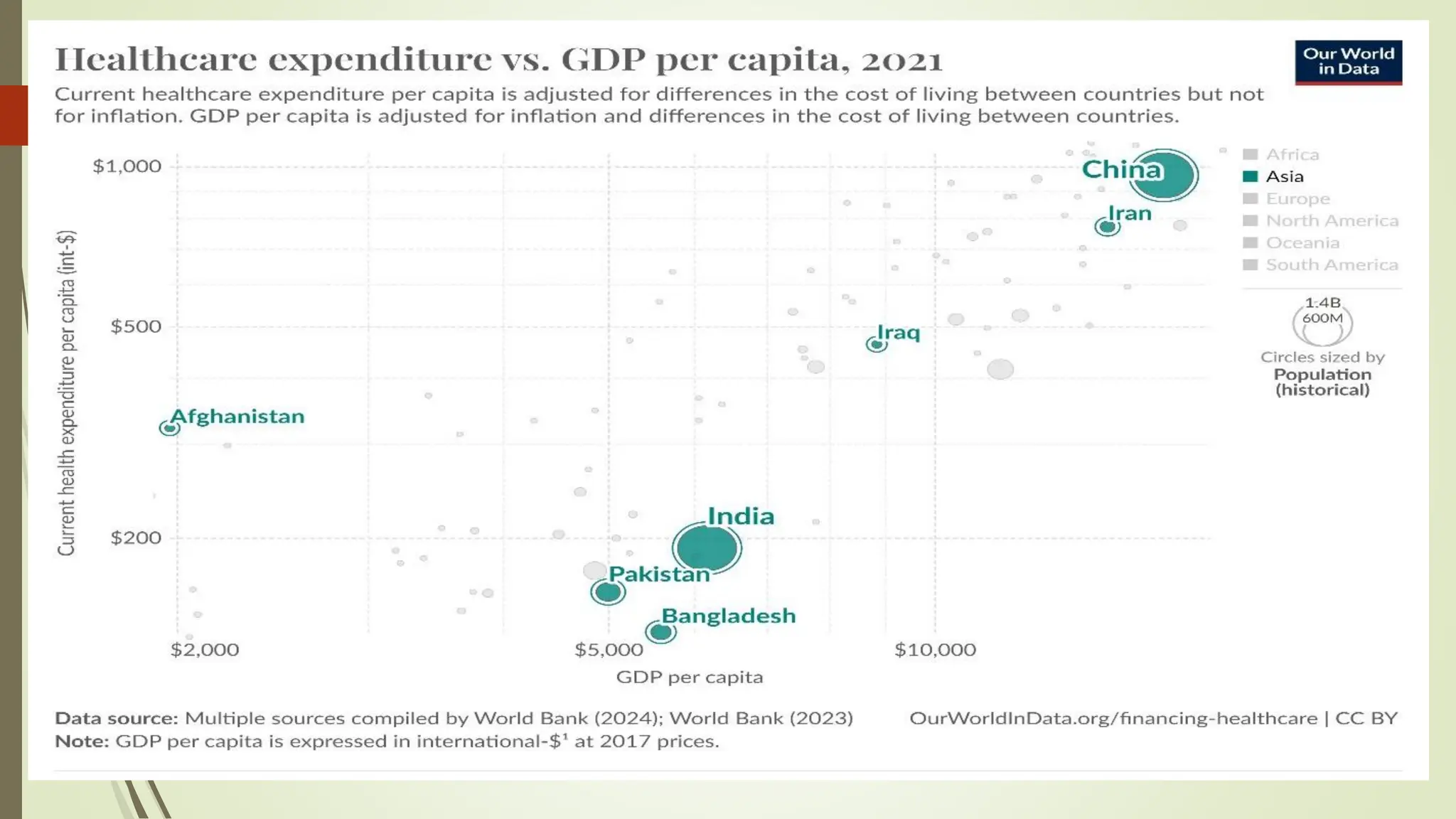
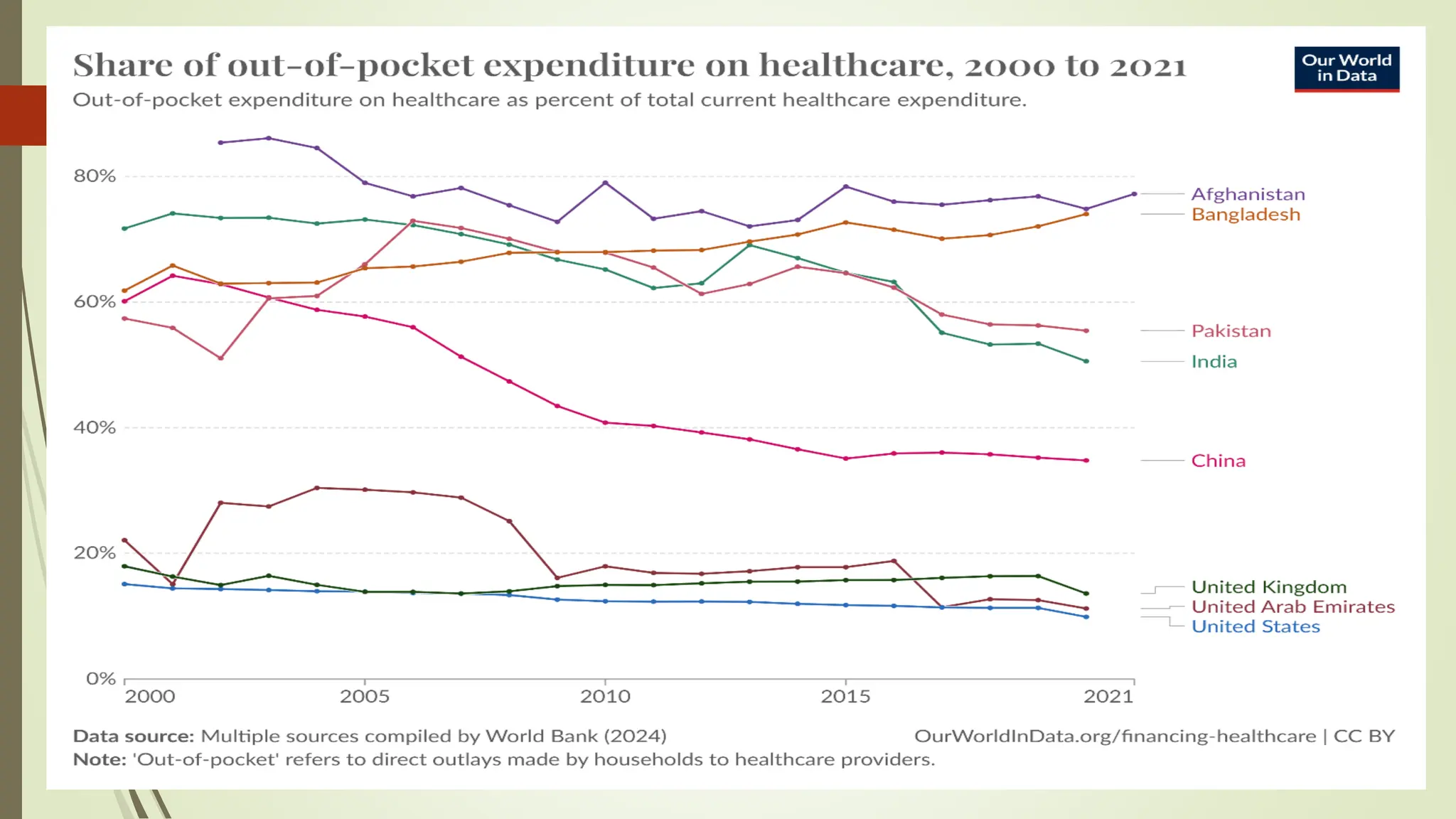
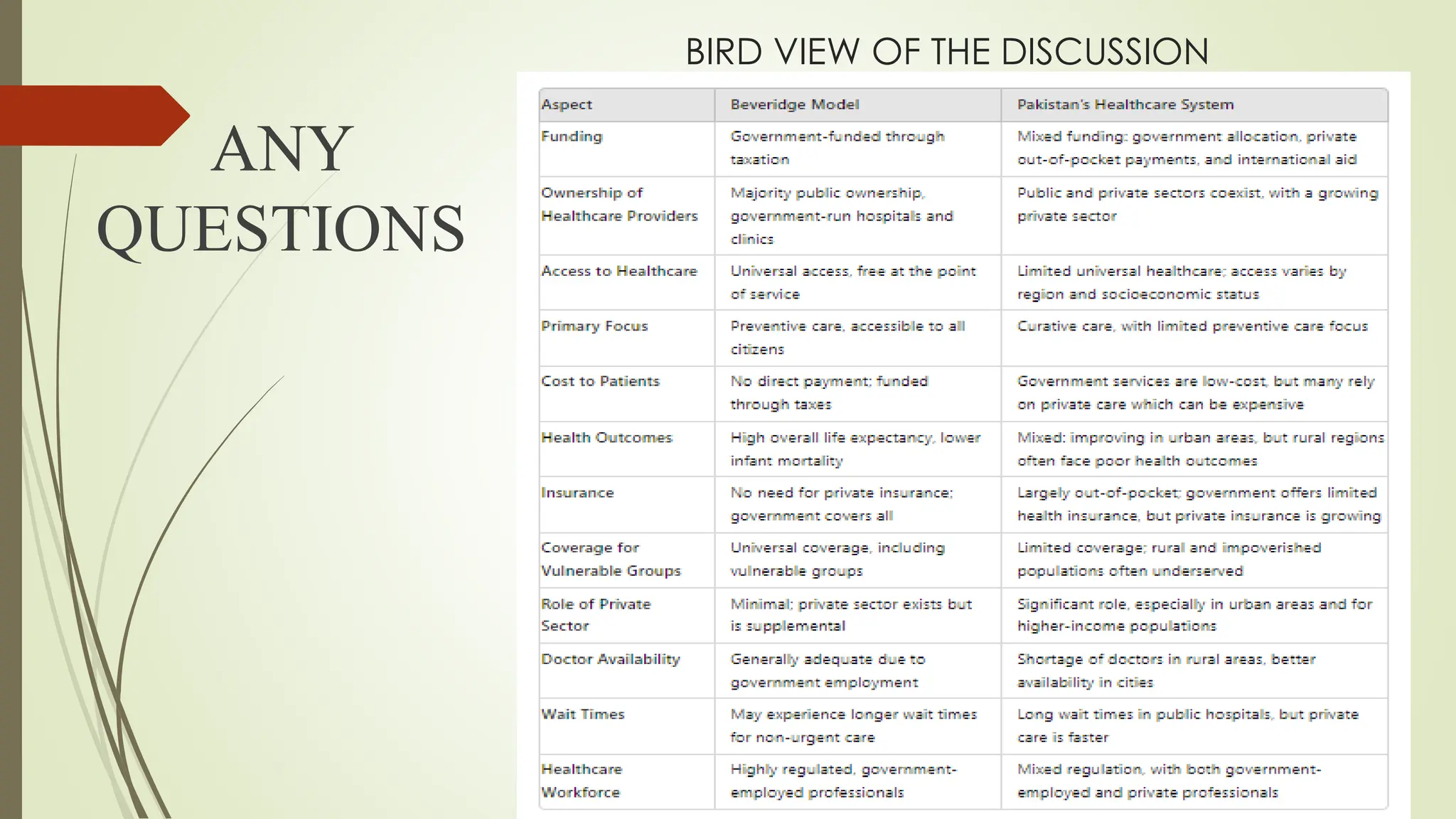
The document compares the Beveridge model of healthcare, emphasizing government-funded universal coverage, with Pakistan's hybrid healthcare system that includes both public and private sectors. While both systems aim for universal access and are government-funded, Pakistan faces challenges due to significant private sector involvement and high out-of-pocket expenses. The analysis points to key differences in funding mechanisms and health outcomes, indicating a need for a nuanced approach to improve healthcare delivery in Pakistan.