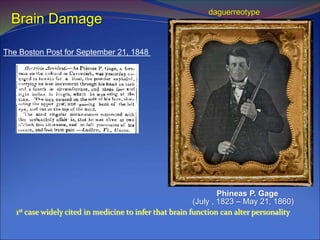
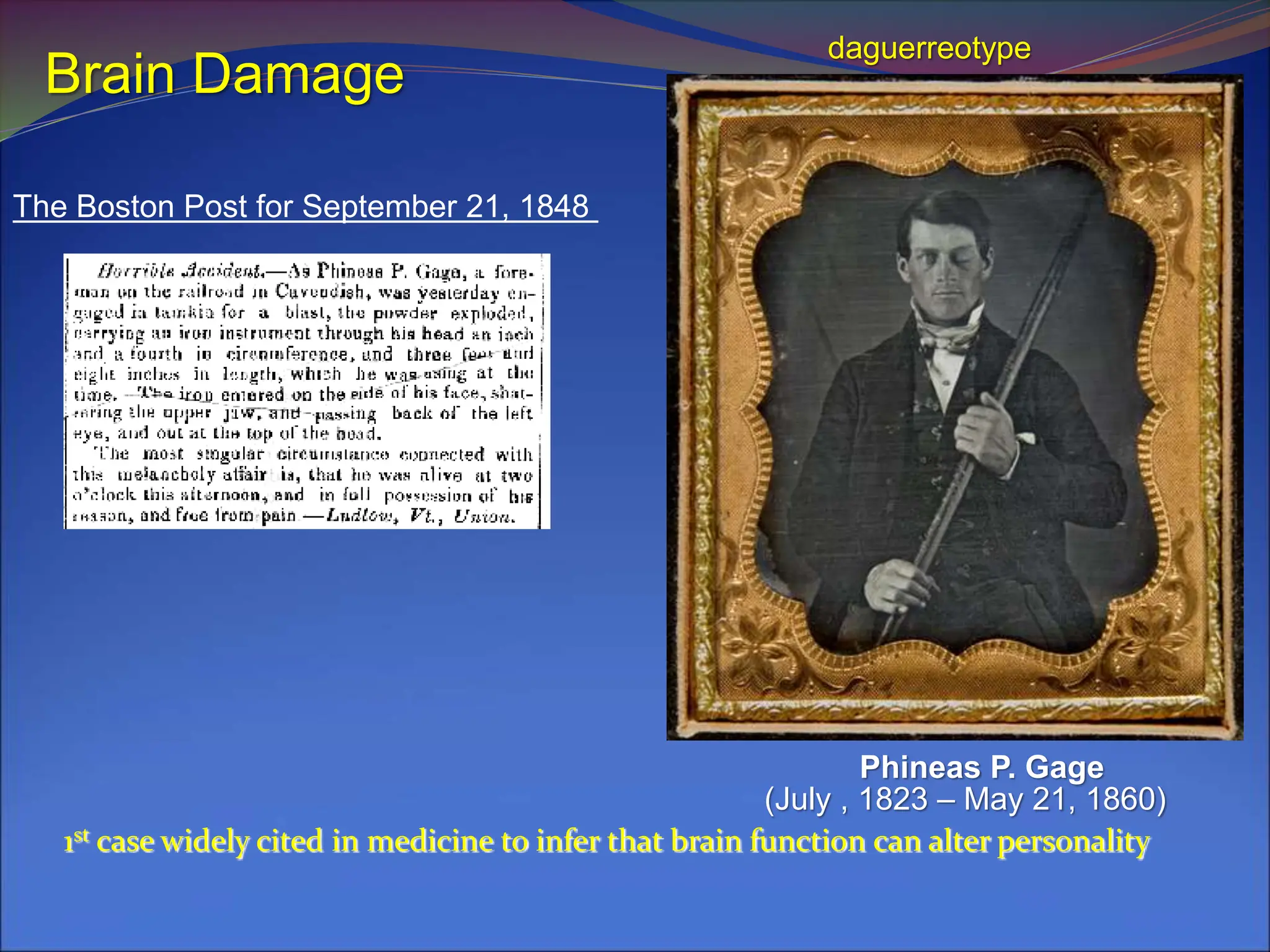
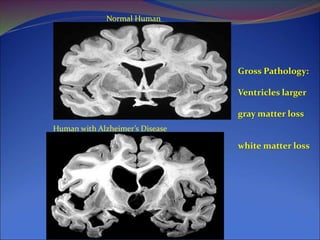
Phineas P. Gage's 1848 case is pivotal in demonstrating how brain damage can significantly alter personality, specifically affecting the frontal cortex and resulting in disinhibited behavior. Traumatic brain injuries (TBI) and neurological disorders like Alzheimer's and Parkinson's disease are discussed, highlighting the causes, symptoms, and impacts of these conditions on individuals. Treatment options, particularly for dementia, include drugs that increase acetylcholine availability, though their effectiveness varies among patients.