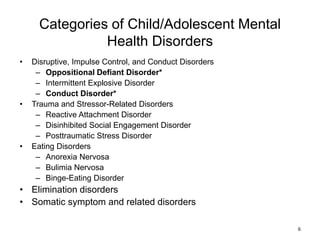
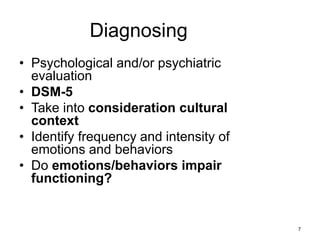
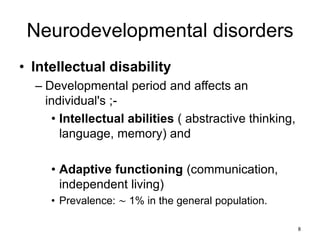
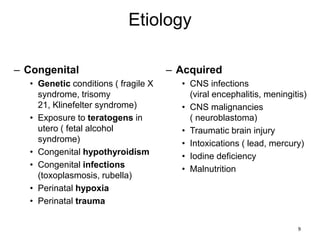
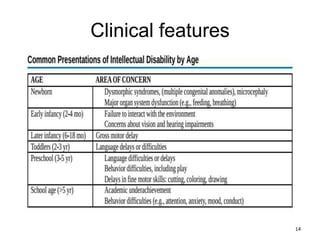
The document discusses several common mental health disorders in children and adolescents. It begins by providing epidemiological data, noting that 11.3% of US children have a mental disorder with ADHD being most prevalent. It then categorizes disorders and provides more detail on selected categories including neurodevelopmental disorders like intellectual disability, autism spectrum disorder, and attention deficit hyperactivity disorder. It discusses symptoms, diagnosis, treatment and prognosis for these conditions. The document also covers anxiety disorders like separation anxiety disorder and selective mutism.

![Epidemiology
• Sex: ♂ > ♀ [1]
• Age of onset: usually before 12 years [2]
• Prevalence: ∼ 5% [1]
27](https://image.slidesharecdn.com/commonpsychiatricdisordershab-231230063844-fc473293/85/common-psychiatric-disorders-hab-pptx-rev-27-320.jpg)