GENUS FEATURES
Gram negativerod
Ferments lactose, which grow pink on mcConkey
agar and the colonies grow with an indescent
green sheen on EMB agar
Catalase positive
Facultative anaerobe
Reservoir: human colon (may colonize
vagina/urethra)
Encapsulated (impedes phagocytosis; colonizing
factor adhesins bind to the mucosa)
4.
DISEASES
The number onecause of urinary tract infections,
endogenous fecal flora contaminate and ascend the
urethra, more common in females because of the
shorter urethras and the mechanism is due to
fimbria/pili that allows for adherence to uroepithelium.
Most common cause of neonatal meningitis. Occurs as
a result of maternal fecal flora contamination during
parturition ( mechanism is through bacterial capsule
that has a K1 serotype antigen)
Septicemia ( gram negative), cause by the LPS
endotoxin.
5.
GASTROENTERITIS
EHEC (enterohemorrahgic strain)
• Come from bovine fecal contamination served in undercooked
meat or at petting zoos
• Causes bloody diarrhea that is not inflammatory (no fever or pus)
• EHEC can be tested on Smac plate because it does not ferment
sorbitol
• The toxin inhibits protein synthesis by interfering with the 60s
ribosomal subunit (shiga like toxin)
• (0157: H7 serotype) in children, EHEC infection may progress to
HUS, which occurs when the bacteriA damages the endothelial
cells in the glomerulus, becoming thrombogenic, which causes
platelets to aggregates and decrease in platelet count, the clumps
of platelets lyse RBCs causing hemolysis
6.
ETEC ( toxigenicstrain)
• Cause of travelers diarrhea
• Transmitted via the fecal oral route through
contaminated water
• Causes explosive watery diarrhea
• Mechanism from two toxins
1. LT (heat labile toxin) which stimulate adenyl
cyclase and
2. ST (heat stable toxin) which stimulate
guanylate cyclase
Both results in increase in chloride and water
into the small intestines.
7.
DIAGNOSIS AND TREATMENT
Diagnosisis by
Immunoassay
DNA probes
Serotyping
PCR
Treatment is supportive and rehydration in
severe cases.
DISEASE
• Salmonella speciescause enterocolitis, enteric fevers such as
typhoid fever, and septicemia with metastatic infections such
as osteomyelitis. They are one of the most common causes of
bacterial enterocolitis in the United States.
10.
IMPORTANT PROPERTIES
Salmonellaeare gram-negative rods that
– do not ferment lactose
– produce H2S—features that are used in their laboratory identification
– Antigenic—cell wall O, flagellar H, and capsular Vi (virulence)
There are two forms of the H antigens; phases 1 and 2
The Vi antigens (capsular polysaccharides) are antiphagocytic and are
an important virulence factor for S. typhi, the agent of typhoid fever.
The Vi antigens are also used for the serotyping of S. typhi in the
clinical laboratory.
11.
Clinically, theSalmonella species are often thought of in two distinct
categories, namely:
– the typhoidal species (i.e., those that cause typhoid fever) and the
– nontyphoidal species (i.e., those that cause diarrhea [enterocolitis] and
metastatic infections, such as osteomyelitis).
The typhoidal species are S. typhi and S.paratyphi. The nontyphoidal
species are the many serotypes of S. enterica.
Of the serotypes, S. enterica serotype choleraesuis is the species
most often involved in metastatic infections.
12.
Pathogenesis & Epidemiology
•The three types of Salmonella infections
(enterocolitis, enteric fevers, and septicemia) have
different pathogenic features.
13.
Pathogenesis & Epidemiology
Enterocolitis is characterized by an invasion of the epithelial and
subepithelial tissue of the small and large intestines. Strains that
do not invade do not cause disease.
The organisms penetrate both through and between the mucosal
cells into the lamina propria, with resulting inflammation and
diarrhea.
Neutrophils limit the infection to the gut and the adjacent
mesenteric lymph nodes; bacteremia is infrequent in enterocolitis.
Gastric acid is an important host defense; gastrectomy or use of
antacids lowers the infectious dose significantly.
14.
Typhoid infectionbegins in the small intestine, but few
gastrointestinal symptoms occur.
• The organisms enter, multiply in the mononuclear phagocytes of
Peyer’s patches, and then spread to the phagocytes of the liver,
gallbladder, and spleen.
• This leads to bacteremia, which is associated with the onset of
fever and other symptoms, probably caused by endotoxin.
• Survival and growth of the organism within phagosomes in
phagocytic cells are a striking feature of this disease, as is the
prediction for invasion of the gallbladder, which can result in
establishment of the carrier state and excretion of the bacteria in
the feces
15.
Septicemia accountsfor only about 5% to 10% of Salmonella infections
and occurs in one of two settings:
• A patient with an underlying chronic disease, such as sickle cell anemia or cancer,
• A child with enterocolitis.
• The septic course is more indolent than that seen with many other
gram-negative rods.
• Bacteremia results in the seeding of many organs, with osteomyelitis,
pneumonia, and meningitis as the most common sequelae.
• Osteomyelitis in a child with sickle cell anemia is an important example
of this type of salmonella infection.
• Previously damaged tissues, such as infarcts and aneurysms, especially
aortic aneurysms, are the most frequent sites of metastatic abscesses.
• Salmonella are also an important cause of vascular graft infections.
16.
S. typhi, thecause of typhoid fever, is transmitted only by
humans, but all other species have a significant animal as
well as human reservoir.
Animal sources;
– poultry and eggs
– meat products that are inadequately cooked
– Dogs and other pets, including turtles, snakes, lizards, and iguanas
17.
Clinical Findings
• Afteran incubation period of 12 to 48 hours
– enterocolitis begins
– nausea and vomiting
– abdominal pain
– diarrhea, which can vary from mild to severe, with or without blood.
HIV-infected individuals, especially those with a low CD4 count, have a
much greater number of Salmonella infections.
In typhoid fever, and in enteric fever, the onset of illness is slow, with fever
and constipation rather than vomiting and diarrhea predominating.
The disease begins to resolve by the third week, but severe
complications such as
– intestinal hemorrhage or perforation can occur.
– become chronic carriers.
18.
LABORATORY DIAGNOSIS
Inenterocolitis, the organism is most easily isolated from a stool sample.
However, in the enteric fevers,
– blood culture during the first 2 weeks of illness.
– Bone marrow cultures
– Stool cultures
Salmonellae form non–lactose-fermenting (colorless) colonies on
MacConkey’s or EMB agar. On TSI agar, an alkaline slant and an acid butt,
frequently with both gas and H2S (black color in the butt), are produced.
S. typhi does not form gas and produces only a small amount of H2S.
Salmonella isolate can be identified and grouped by the slide
agglutination test into serogroup A, B, C, D, or E based on its O antigen.
19.
TREATMENT
Enterocolitis causedby Salmonella is usually a self-limiting
Fluid and electrolyte replacement may be required.
Antimicrobial agents are indicated only for neonates or persons with chronic
diseases who are at risk for septicemia and disseminated abscesses
The treatment of choice for enteric fevers such as typhoid fever and septicemia
with metastatic infection is either ceftriaxone or ciprofloxacin.
Ampicillin or ciprofloxacin should be used in patients who are chronic carriers
of S. typhi.
Cholecystectomy may be necessary to abolish the chronic carrier state.
Focal abscesses should be drained surgically when feasible.
20.
PREVENTION
Salmonella infectionsare prevented mainly by;
– public health and personal hygiene measures.
– Proper sewage treatment
– handwashing prior to food handling
– pasteurization of milk
– proper cooking of poultry, eggs, and meat are all important.
Two vaccines are available;
– One contains the Vi capsular polysaccharide of S. typhi (given intramuscularly),
– the other contains a live, attenuated strain (Ty21a) of S. typhi given orally
The two vaccines are equally effective. The vaccine is recommended for those
who will travel or reside in high-risk areas and for those whose occupation
brings them in contact with the organism
DISEASE
• Shigella speciescause enterocolitis. Enterocolitis caused by Shigella is
often called bacillary dysentery. The term dysentery refers to bloody
diarrhea.
23.
IMPORTANT PROPERTIES
Shigellaeare non–lactose-fermenting, gram-negative rods
that can be distinguished from salmonellae by three criteria:
– They produce no gas from the fermentation of glucose,
– They do not produce H2S
– They are nonmotile.
All shigellae have O antigens (polysaccharide) in their cell
walls, and these antigens are used to divide the genus into
four groups: A, B, C, and D.
24.
PATHOGENESIS AND EPIDEMIOLOGY
Shigellae are the most effective pathogens among the enteric bacteria. They
have a very low ID50. Ingestion of as few as 100 organisms causes disease,
whereas at least 105 V. cholerae or Salmonella organisms are required to
produce symptoms.
Shigellosis is only a human disease (i.e., there is no animal reservoir).
The organism is transmitted by the fecal–oral route. The four Fs—fingers, flies,
food, and feces—are the principal factors in transmission.
Foodborne outbreaks outnumber waterborne outbreaks by 2 to 1. Outbreaks
occur in day care nurseries and in mental hospitals, where fecal–oral
transmission is likely to occur.
Children younger than 10 years account for approximately half of Shigella-
positive stool cultures.
There is no prolonged carrier state with Shigella infections, unlike that seen
with S. typhi infections.
25.
Shigellae, whichcause disease almost exclusively in the
gastrointestinal tract, produce bloody diarrhea (dysentery) by
invading the cells of the mucosa of the distal ileum and colon. Local
inflammation accompanied by ulceration occurs, but the organisms
rarely penetrate through the wall or enter the bloodstream, unlike
salmonellae.
Although some strains produce an enterotoxin (called Shiga toxin),
invasion is the critical factor in pathogenesis. The evidence for this is
that mutants that fail to produce enterotoxin but are invasive can still
cause disease, whereas noninvasive mutants are nonpathogenic.
Shiga toxins are encoded by lysogenic bacteriophages. Shiga toxins
very similar to those produced by Shigella are produced by
enterohemorrhagic E. coli O157:H7 strains that cause enterocolitis
and HUS.
26.
CLINICAL FINDINGS
Afteran incubation period of 1 to 4 days, symptoms begin with fever and abdominal cramps,
followed by diarrhea, which may be watery at first but later contains blood and mucus.
The disease varies from mild to severe depending on two major factors:
– the species of Shigella
– the age of the patient, with young children and elderly people being the most severely affected.
Shigella dysenteriae, which causes the most severe disease, is usually seen in the
United States only in travelers returning from abroad.
Shigella sonnei, which causes mild disease, is isolated from approximately 75% of all
individuals with shigellosis in the United States.
The diarrhea frequently resolves in 2 or 3 days; in severe cases, antibiotics can shorten
the course. Serum agglutinins appear after recovery but are not protective because
the organism does not enter the blood.
The role of intestinal IgA in protection is uncertain.
27.
LABORATORY DIAGNOSIS
Shigellaeform non–lactose-fermenting (colorless) colonies on
MacConkey’s or EMB agar.
On TSI agar, they cause an alkaline slant and an acid butt, with no gas
and no H2S.
Confirmation of the organism as Shigella and determination of its
group are done by slide agglutination.
One important adjunct to laboratory diagnosis is a methylene blue
stain of a fecal sample to determine whether neutrophils are present.
If they are found, an invasive organism such as Shigella, Salmonella,
or Campylobacter is involved rather than a toxin-producing organism
such as V. cholerae, E. coli, or Clostridium perfringens.
28.
TREATMENT
The maintreatment for shigellosis is fluid and electrolyte
replacement. In mild cases, no antibiotics are indicated.
In severe cases
– fluoroquinolone (e.g., ciprofloxacin) is the drug of choice, but the incidence of
plasmids conveying multiple drug resistance is high enough that antibiotic
sensitivity tests must be performed.
– Trimethoprim-sulfamethoxazole is an alternative choice.
Antiperistatical drugs are contraindicated in shigellosis, because they
prolong the fever, diarrhea, and excretion of the organism.
29.
PREVENTION
Prevention ofshigellosis is dependent on interruption of fecal–oral
transmission by;
– proper sewage disposal
– chlorination of water
– personal hygiene (handwashing by food handlers).
There is no vaccine, and prophylactic antibiotics are not
recommended
GENUS FEATURES
Gram negative,curved/comma-shaped rods
with flagella
Oxidase positive
Grows in alkaline environments (does not
particularly like acidic environment) ACID LABILE
Grows on thiosulfate citrate bile salt sucrose
medium (TCB) and turns orange--- ferments
sucrose.
32.
VIBRIO CHOLERAE
The 01serotype and it has been subdivided into
an EL TOR subtype and a CHOLERA subtype.
Distinguishing features: “shooting star”
motility inactivated by specific serum
Reservoir: human colon, can be transiently
carried by shellfish contaminated in water, but
not true reservoirs; human carriage may
persist after untreated infection for months
after infection, but permanent carrier state is
rare.
33.
Transmission is viafecal-oral spread,
transmission requires a high dose because
cholera is sensitive to acid, many will die but
the few will infect.
34.
PATHOGENESIS
Motility, mucinase andtoxin coregulated pili (TCP)
aid in attachment to the intestinal mucosa. There
the enterotoxin choleragen (similar to ETEC’s LT
toxin) activates Gs alpha by ADP ribosylation, which
activates adenylates cyclase , which increases cAMP
causing an efflux of Cl and water into the small
intestines; this leads to rice water diarrhea and
tremendous fluid loss of up to 20L lost and
hypovolemic shock is a major complication if not
treated.
35.
TREATMENT:
• fluid andelectrolyte replacement by IV
• Antibiotics doxycycline or ciprofloxacine can
shorten disease and reduce carriage; resistance to
tetracycline has been reported
PREVENTION
• Proper sanitation
VIBRIO PARAHAEMOLYTICUS AND VIBRIO
VULNIFICUS: both are transmitted by
consumption of raw seafood and cause watery
diarrhea as well.
VIBRIO VULNIFICUS can also cause rapidly
spreading cellulitis that may be difficult to treat.
GENUS: CAMPYLOBACTER
Genus Features
•Gram-negative curved rods with polar
flagella ("gulls' wings")
• Oxidase-positive
Species of Medical Importance - Campylobacter
jejuni
38.
Campylobacter jejuni
Distinguishing Features--microaerophilic,grows well at 42.0°C
on selective media (Campy medium or Skirrow agar)
Reservoir-intestinal tracts of humans, cattle, sheep, dogs, cats,
poultry
Transmission- fecal-oral, primarily from poultry
39.
Pathogenesis
• Low infectiousdose (as few as 500)
• Invades mucosa of the colon, destroying
mucosal surfaces; blood and pus in stools
(inflammatory diarrhea)
• Rarely penetrates to cause septicemia
40.
Disease
• Gastroenteritis -Common cause of infectious
diarrhea worldwide
-In U.S., Campylobacter enteritis > (Salmonella
plus Shigella)
- Ten or more stools/ day, may be frankly bloody
- Abdominal pain, fever, malaise, nausea, and
vomiting
-Generally self-limiting in 3-5 days but may last
longer
41.
- Complications
• Guillain-Barresyndrome (GBS)→ 30% of the
GBS in the U.S. Serotype 0:19, antigenic cross-
reactivity between Campylobacter
oligosaccharides and glycosphingolipids on
neural tissues
• Reactive arthritis
42.
Diagnosis
• Culture onCampylobacter or Skirrow agar at 42°C
Treatment
• Mostly supportive via fluid and electrolyte replacement
• Erythromycin, fluoroquinolones, penicillin resistant
Prevention
• There is no vaccine or other specific preventive
measure. Proper sewage disposal and personal
hygiene (handwashing) are important.
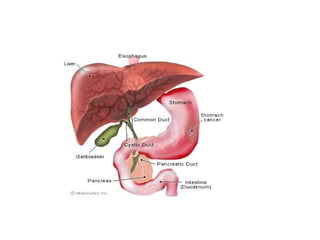
Historical Background
Human stomachlong considered inhospitable for bacteria.
Spiral shaped organisms occasionally visualized in gastric mucous
layer, but no evidence of disease association.
1982 - Marshall and Warren identified and subsequently cultured
the gastric bacterium, Campylobacter pyloridis, later reclassified as
Helicobacter pylori.
Discovery revolutionized the treatment of duodenal and gastric
ulcers.
Earned them the Nobel Prize for Medicine in
2005. Nearly 20 species of Helicobacter are now
recognized.
The gastric helicobacters colonise the stomachs of
animals. The monkey, cat, dog, tiger all harbour their own
species.
45.
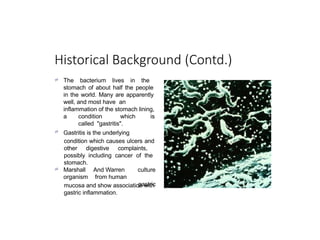
Historical Background (Contd.)
The bacterium lives in the
stomach of about half the people
in the world. Many are apparently
well, and most have an
inflammation of the stomach lining,
a condition which is
called "gastritis".
Gastritis is the underlying
condition which causes ulcers and
other digestive complaints,
possibly including cancer of the
stomach.
Marshall
organism
And Warren
from human
culture
gastric
mucosa and show association with
gastric inflammation.
46.
A silver stainof H. pylori on gastric mucus-secreting epithelial cells
(x1000). From Dr. Marshall's stomach biopsy taken 8 days after he
drank a culture of H. pylori (1985).
47.
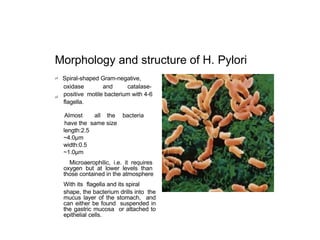
Morphology and structureof H. Pylori
Spiral-shaped Gram-negative,
oxidase and catalase-
positive motile bacterium with 4-6
flagella.
Almost all the bacteria
have the same size
length:2.5
~4.0μm
width:0.5
~1.0μm
Microaerophilic, i.e. it requires
oxygen but at lower levels than
those contained in the atmosphere
With its flagella and its spiral
shape, the bacterium drills into the
mucus layer of the stomach, and
can either be found suspended in
the gastric mucosa or attached to
epithelial cells.
48.
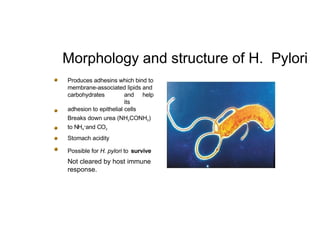
Morphology and structureof H. Pylori
Produces adhesins which bind to
membrane-associated lipids and
carbohydrates and help
its
adhesion to epithelial cells
Breaks down urea (NH2CONH2)
to NH4
+
and CO2
Stomach acidity
Possible for H. pylori to survive
Not cleared by host immune
response.
49.
Epidemiology
The most commonchronic bacterial infection in humans.
The risk of acquiring H. pylori infection is related to socio-economic
status and living conditions early in life.
Developing nations: the majority of children are infected before the
age of 10, the prevalence in adults peaks at more than 80 percent
before age 50.
Developed countries: evidence of infection in children is unusual but
becomes more common during adulthood.
Immigration is responsible for isolated areas of high revalence in
some Western countries.
50.
Transmission of H.pylori
Transmission— Route by which
infection occurs remains unknown
Humans are major
source of
- if not
only–
transmissio
n reservoir.
Transmissio
n
sharing the
among
same
persons
living
environment.
Family members often carry same
strain.
Person-to-person transmission of
H. pylori through either fecal/oral
or oral/oral exposure seems most
likely.
Organism can be cultured from
feces.
Infection from environment or from
animals cannot be totally
excluded.
51.
Defense mechanism
of
H.pylori
OnceH. pylori is ensconced in the
mucus, it is able to fight the
stomach acid that does reach it
with an enzyme called urease.
Urease converts urea, of which
there is an abundant supply in the
stomach (from saliva and gastric
juices), into bicarbonate and
ammonia, which are strong bases.
This creates a cloud of acid
neutralizing chemicals around the
H. pylori, protecting it from the
acid in the stomach.
The reaction of urea hydrolysis is
important for diagnosis of H.pylori
by the breath test.
52.
Site of infection
•
•
•
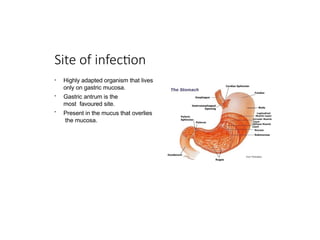
Highlyadapted organism that lives
only on gastric mucosa.
Gastric antrum is the
most favoured site.
Present in the mucus that overlies
the mucosa.
53.
Pathogenesis
•Most bacteria arekilled in hostile environment of gastric lumen.
•H. pylori proliferates in mucus layer over epithelium and is not cleared by host immune response.
•Pathophysiology of H. pylori infection and its eventual clinical outcome is a complex interaction between the host and the
bacterium.
•H. pylori survives and grows there because of a variety of virulence factors that contribute to gastric inflammation, alter gastric
acid production, and cause tissue destruction.
Flagella - allows penetration of H.pylori into gastric mucous layer. Adhesins - mediate binding to host cells.
Localized tissue damage mediated by:
Mucinases and phospholipases - disrupt gastric mucus
Vacuolating cytotoxin - induces vacuolation in epithelial cells that results in epithelial cell damage
54.
Symptoms of H.pyloriinfection
Abdominal pain with burning
or gnawing sensation.
With empty stomach; pain is
often made worse
Night time pain is
common.
Poor appetite.
Weight loss.
Heartburn.
Indigestion (dyspepsia)
Belching.
Nausea.
Vomiting.
Blood in stool.
55.
Diseases associated with
H.Pylori
•
•
•
•
•
•
Duodenal Ulcer
Gastric (Stomach) Ulcer
Non-Ulcer dyspepsia
Weird Syndromes (associated with acne
rosacea, gulf veterans syndrome, chronic
fatigue syndrome and chronic halitosis)
Stomach
Cancer MALT
Lymphoma
58.
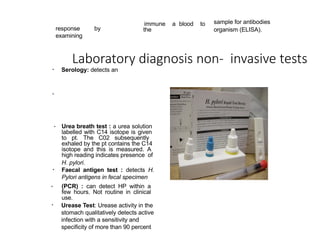
Laboratory diagnosis non-invasive tests
• Serology: detects an
response by
examining
immune a blood to
the
sample for antibodies
organism (ELISA).
•
• Urea breath test : a urea solution
labelled with C14 isotope is given
to pt. The C02 subsequently
exhaled by the pt contains the C14
isotope and this is measured. A
high reading indicates presence of
H. pylori.
Faecal antigen test : detects H.
Pylori antigens in fecal specimen
•
(PCR) : can detect HP within a
few hours. Not routine in clinical
use.
Urease Test: Urease activity in the
stomach qualitatively detects active
infection with a sensitivity and
specificity of more than 90 percent
59.
Invasive testing
Histological examinationof biopsy specimens
of gastric/duodenal mucosa take a endoscopy
Culture
Not sensitive then a skilled microscopy histological section
Can be used for antibiotic resistance testing
Requires selected agars and incubation periods
Treatment and Prevention
Treatmentof duodenal ulcers with antibiotics e.g. amoxicillin and
metronidazole, and bismuth salts (Pepto-Bismol) results in a greatly
decreased recurrence rate.
Tetracycline can be used instead of amoxicillin .
There is no vaccine or other specific preventive measure .
62.
Conclusion
A characteristic ofH. pylori infection in humans is gastritis, which persists for
decades without causing serious damage in most cases.
The clinical complications of H. pylori infection, such as peptic ulcer
disease and gastric cancer, appear to represent an imbalance in gastric
homeostasis.
IMPORTANT PROPERTIES
Thesegram-negative rods are distinguished from other members of the
Enterobacteriaceae by their ability to produce the enzymes;
– phenylalanine deaminase.
– urease, which cleaves urea to form NH3 and CO2. Certain species are very
motile and produce a striking swarming effect on blood agar, characterized by
expanding rings (waves) of organisms over the surface of the agar.
The cell wall O antigens of certain strains of Proteus, such as OX-2, OX-19, and
OX-K, cross-react with antigens of several species of rickettsiae. These Proteus
antigens can be used in laboratory tests to detect the presence of antibodies
against certain rickettsiae in patients’ serum. This test, called the Weil-Felix
reaction after its originators, is being used less frequently as more specific
procedures are developed.
65.
In thepast, there were four medically important species of Proteus. However, molecular
studies of DNA relatedness showed that two of the four were significantly different. These
species have been renamed:
– Proteus morganii is now Morganella morganii
– Proteus rettgeri is now Providencia rettgeri
– Proteus vulgaris
– Proteus mirabilis
In the clinical laboratory, these organisms are distinguished on the basis of several
biochemical tests.
66.
PATHOGENESIS
The organismsare present in the human colon as well as in soil and water.
Their tendency to cause urinary tract infections is probably due to their
presence in the colon and to colonization of the urethra, especially in
women. The vigorous motility of Proteus organisms may contribute to their
ability to invade the urinary tract.
Production of the enzyme urease is an important feature of the
pathogenesis of urinary tract infections by this group.
– Urease hydrolyzes the urea in urine to form ammonia, which raises the pH, producing an
alkaline urine. This encourages the formation of stones (calculi) called “struvite” composed of
magnesium ammonium phosphate. Stones in the urinary tract obstruct urine flow, damage
urinary epithelium, and serve as a nidus for recurrent infection by trapping bacteria within the
stone. Because alkaline urine also favors growth of the organisms and more extensive renal
damage, treatment involves keeping the urine at a low pH.
67.
CLINICAL FINDINGS
Thesigns and symptoms of urinary tract infections caused by these organisms cannot
be distinguished from those caused by E. coli or other members of the
Enterobacteriaceae.
Proteus species can also cause
– Pneumonia
– wound infections
– septicemia.
P. mirabilis is the species of Proteus that causes most community and hospital-
acquired infections
P. rettgeri is emerging as an important agent of nosocomial infections.
68.
LABORATORY DIAGNOSIS
Theseorganisms usually are highly motile and produce a “swarming” overgrowth on blood
agar, which can frustrate efforts to recover pure cultures of other organisms.
Growth on blood agar containing phenylethyl alcohol inhibits swarming, thus allowing
isolated colonies of Proteus and other organisms to be obtained. They produce non–
lactose-fermenting (colorless) colonies on MacConkey’s or EMB agar.
P. vulgaris and P. mirabilis produce H2S, which blackens the butt of TSI agar, whereas
neither M. morganii nor P. rettgeri does.
P. mirabilis is indole-negative, whereas the other three species are indole-positive—a
distinction that can be used clinically to guide the choice of antibiotics.
These four medically important species are urease-positive. Identification of these
organisms in the clinical laboratory is based on a variety of biochemical reactions.
69.
TREATMENT
Most strainsare sensitive to
– aminoglycosides
– trimethoprim-sulfamethoxazole,
But because individual isolates can vary, antibiotic sensitivity tests should be
performed. P. mirabilis is the species most frequently sensitive to ampicillin. The
indole-positive species (P. vulgaris, M. morganii, and P. rettgeri) are more resistant
to antibiotics than is P. mirabilis, which is indole-negative.
The treatment of choice for the indole-positive species is a cephalosporin (e.g.,
cefotaxime).
P. rettgeri is frequently resistant to multiple antibiotics.
70.
PREVENTION
• There areno specific preventive measures, but many hospital-acquired urinary tract
infections can be prevented by prompt removal of urinary catheters.
GENUS: PSEUDOMONAS
Genus Features
•Gram-negative rod
• Oxidase-positive as oxidation involves elctron transport by cytochrome
• Aerobic (non-fermenting)
Species of Medical Importance-Pseudomonas aeruginosa
• Pseudomonas aeruginosa
Distinguishing Features
• Oxidase-positive, Gram-negative rods, non-fermenting (derive their energy only by oxidation of sugars rather than by fermentation )
•Produces two pigments : Pyocyanin (blue-green) which can colour the pus in a wound blue and pyoverdin(fluorescein),a yellow-green
pigment that fluoresces under ultraviolet light, a property that can be used in the early detection of skin infection in burn patients
• Grape-like odor
• Strains of P. eruginosa isolated from cystic fibrosis patients have a prominent slime layer (glycocalyx), which gives their colonies a very
mucoid appearance.
The slime layer mediates adherence of the organism to mucous membrane of the respiratory tract and prevents antibody from binding
to the organism.
• Non-lactose-fermenting colonies on EMB or MacConkey
72
73.
• Reservoir
Found chielyin soil and water ,although approximately 10% of people carry it in the normal flora of
the colon.
It is found on the skin in moist areas and can colonize the upper respiratory tract of hospitalized
patients.
• Transmission-water aerosols, raw vegetables, flowers
• Pathogenesis
Based on various virulence
• Endotoxin causes inflammation in tissues and causes the symptoms of sepsis and septic shock.
• Pseudomonas exotoxin A: causes tissue necrosis
ADP ribosylates elongation factor 2 , inhibiting protein synthesis (like diphtheria toxin)
• It produces enzymes such as elastase and protease, which are hisotoxic and facilitate invasion of
the organism into the blood stream
Pyocyanin damages the cilia and mucosal cells of the respiratory tract
73
74.
Disease(s)
• Healthy people
-Transient gastrointestinal tract colonization: loose stools (10%
population) Hot tub folliculitis
- Eye ulcers: trauma, coma, or prolonged contact wear
• Burn patients
-Gastrointestinal tract colonization → skin → colonization of
eschar→ cellulitis (blue-green pus) → septicemia
74
75.
Diagnosis
-Gram stain andculture
Treatment -antipseudomonal penicillin eg ticarcillin or piperacilin and
an aminoglycoside eg gentamicin or amikacin
Prevention
• Pasteurization or disinfection of water-related equipment, hand
washing; prompt removal of catheters
• No flowers or raw vegetables in burn units
75
76.
BACTEROIDES & PREVOTELLA
Diseases
•Members of the genus Bacteroides are the most
common cause of serious anaerobic infections (e.g.
sepsis, peritonitis and abscesses). Bacteroides fragilis
is the most frequent pathogen.
• Prevotella melaninogenica is also an important
pathogen. P.
melaninogenica was formerly known as Bacteroides
melaninogenicus, and both names are still encountered.
77.
Important Properties
• Bacteroidesand Prevotella organisms are anaerobic, non–
spore-forming, gram negative rods. Of the many species
of bacteroides, two are human pathogen: B. fragilis7 and
Bacteroides corrodens.
• Members of the B. fragilis group are the predominant
organisms in the human colon, numbering approximately
1011/g of feces, and are found in the vagina of
approximately 60% of women. P. melaninogenica and B.
corrodens occur primarily in the oral cavity.
78.
Pathogenesis & Epidemiology
•Because Bacteroides and Prevotella species are part of the normal flora,
infections are endogenous, usually arising from a break in a mucosal surface,
and are not communicable. These organism cause a variety of infections, such
as local abscesses at the site of a mucosal break, metastatic abscesses by
hematogenous, spread to distant organs, or lung abscesses by aspiration of oral
flora.
• Predisposing factors such as surgery, trauma, and chronic disease play an
important role in pathogenesis. Local tissue necrosis, impaired blood supply,
and growth of facultative anaerobes at the site contribute to anaerobic
infections. The facultative anaerobes, such as E. coli, utilize the oxygen, thereby
reducing it to a level that allows the anaerobic Bacteroides and Prevotella
strains to grow. As a result, many anaerobic infections contain a mixed
facultative and anaerobic flora. This has important implications for therapy;
both the facultative anaerobes and the anaerobes should be treated.
79.
Clinical Findings
• TheB. fragilis group of organisms is most frequently associated
with intraabdominal infections, either peritonitis or localized
abscesses. Pelvic abscesses, necrotizing fasciitis, and bacteremia
occur as well. Abscesses of the mouth, pharynx, brain, and lung
are more commonly caused by P. melaninogenica, a member of
the normal oral flora, but B. fragilis is found in about 25% of
lung abscesses.
• In general,B fragilis causes disease below the diaphragm,
whereas P. melaninogenica causes disease above the
diaphragm. Prevotella intermedia is an important cause of
gingivitis, periodontitis, and dental abscess.
80.
Laboratory Diagnosis
• Bacteroidesspecies can be isolated anaerobically on
blood agar plates containing kanamycin and
vancomycin to inhibit unwanted organisms.
• They are identified by biochemical reactions (e.g.,
sugar fermentations) and by production of certain
organic acids (e.g., formic, acetic, and propionic acids),
which are detected by gas chromatography. P.
melaninogenica produces characteristic black colonies.
81.
Treatment
• Members ofthe B. fragilis group are resistant to penicillins, first-
generation cephalosporins, and aminoglycosides, making them
among the most antibiotic resistantof the anaerobic bacteria.
Penicillin resistance is the result of β-lactamase production.
• Metronidazole is the drug of choice, with cefoxitin, clindamycin,
and chloramphenicol as alternatives. Aminoglycosides are
frequently combined to treat the facultative gram-negative rods in
mixed infections. The drug of choice for P.melaninogenica
infections is either metronidazole or clindamycin. β-Lactamase–
producing strains of P. melaninogenica have been isolated from
patients. Surgical drainage of abscesses usually accompanies
antibiotic therapy, but lung abscesses often heal without drainage.
82.
Prevention
• Prevention ofBacteroides and Prevotella
infections centers on perioperative
administration of a cephalosporin, frequently
cefoxitin, for abdominal or pelvic surgery.
There is no vaccine.

![ Clinically, the Salmonella species are often thought of in two distinct
categories, namely:
– the typhoidal species (i.e., those that cause typhoid fever) and the
– nontyphoidal species (i.e., those that cause diarrhea [enterocolitis] and
metastatic infections, such as osteomyelitis).
The typhoidal species are S. typhi and S.paratyphi. The nontyphoidal
species are the many serotypes of S. enterica.
Of the serotypes, S. enterica serotype choleraesuis is the species
most often involved in metastatic infections.](https://image.slidesharecdn.com/8-260125133929-89f0c7c7/85/Common-Gram-Negative-Rod-Enteric-Tract-infection-ppt-11-320.jpg)