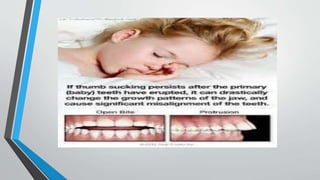
Common behavioral problems in school children include habit disorders like thumb sucking and nail biting, speech disorders like stammering, eating disorders like pica, sleep disorders, and personality disorders. These problems are often due to developmental delays, stress, genetics, family dynamics, or other psychological factors. Teachers and parents should identify problems early based on how behaviors affect functioning. Management involves addressing underlying causes through counseling, behavioral therapy, ensuring proper sleep/nutrition, and creating a supportive environment. Medication may help in some severe or resistant cases. The document provides examples and treatment approaches for various common behavioral issues in school-aged children.