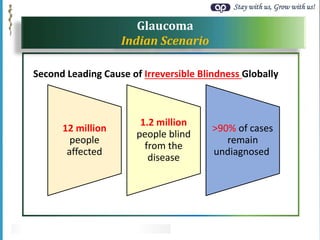
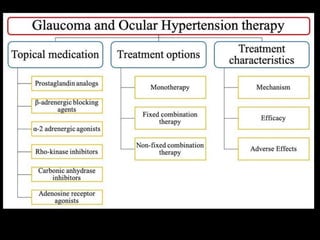
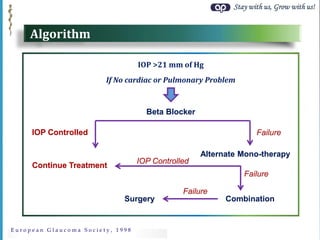
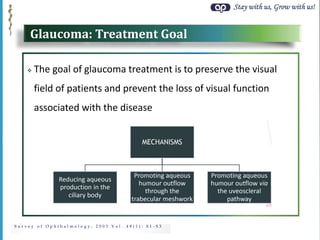
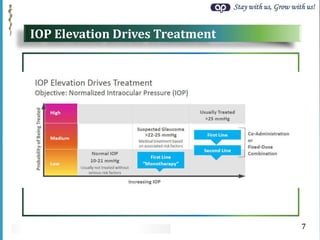
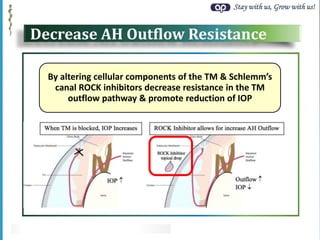
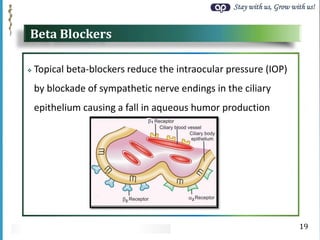
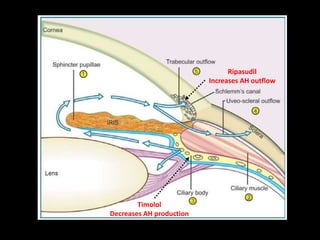
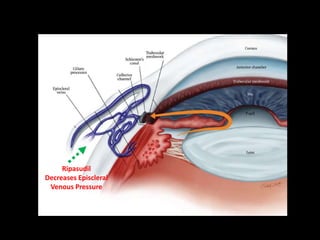
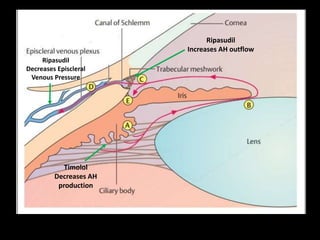
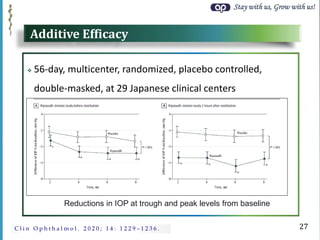
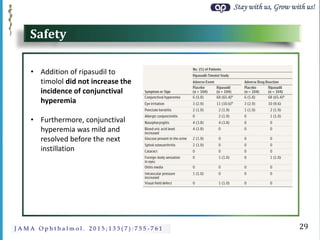
The document discusses combination therapy for glaucoma management using ripasudil and timolol. It provides background on glaucoma prevalence in India. It outlines the standard treatment algorithm and rationale for combination therapy when monotherapy fails to control intraocular pressure. The document reviews evidence that combination therapy provides better IOP control than monotherapy. It describes the mechanisms of action, efficacy, and safety of ripasudil and timolol as well as clinical trial results demonstrating the additive IOP-lowering effects of the combination.