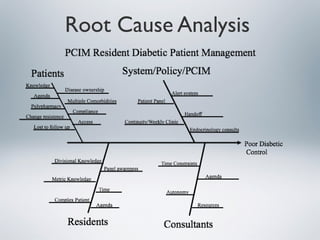
This document outlines a quality improvement project to improve diabetes management in a primary care clinic. It notes that diabetic patients in the clinic are not meeting quality goals for HbA1c, LDL, and blood pressure. The project will test the effectiveness of providing quarterly reports on these measures and one-on-one care manager meetings (the intervention) versus usual care. The intervention aims to increase residents' awareness of clinical guidelines and engage patients. Project outcomes will assess the metrics over time and resident/care manager satisfaction to determine if the intervention is effective and worthwhile.