This study evaluates the quality and cost performance of the Daily Planet Healthcare Center, an FQHC in Richmond, VA, from 2012-2014. The clinic serves high-risk, underserved, and uninsured populations including those experiencing homelessness. The study found that the clinic improved quality measures for preventative services after becoming a level 3 Patient-Centered Medical Home in 2013. Chronic disease management measures were steady over the period. While the clinic's total cost per patient was higher than the state, it was lower than national costs and its total cost per visit was much lower than state and national costs.
Uncover Hidden Population Using Predictive Modeling Tool VitreosHealth
Using Predictive Modeling Tool to Identify at Risk Patients who has a chance of becoming users of High-Cost Healthcare service and subsequently Reducing PMPM (Per Member Per Month) Costs While Increasing Member Satisfaction
Weitzman 2013: State Health Policy Initiatives as Drivers for Improving Care...CHC Connecticut
Sue Birch presents on State Health Policy Initiatives as Drivers for Improving Care Outcomes: Colorado's Accountable Care Collaborative at the 2013 Weitzman Symposium
March 02, 2018
Value-based health care is one of the most pressing topics in health care finance and policy today. Value-based payment structures are widely touted as critical to controlling runaway health care costs, but are often difficult for health care entities to incorporate into their existing infrastructures. Because value-based health care initiatives have bipartisan support, it is likely that these programs will continue to play a major role in both the public and private health insurance systems. As such, there is a pressing need to evaluate the implementation of these initiatives thus far and to discuss the direction that American health care financing will take in the coming years.
To explore this important issue, the Petrie-Flom Center for Health Law Policy, Biotechnology, and Bioethics at Harvard Law School collaborated with Ropes & Gray LLP to host a one-day conference on value-based health care. This event brought together scholars, health law practitioners, and health care entities to evaluate the impact of value-based health care on the American health care system.
For more information, visit our website at: http://petrieflom.law.harvard.edu/events/details/will-value-based-care-save-the-health-care-system
Uncover Hidden Population Using Predictive Modeling Tool VitreosHealth
Using Predictive Modeling Tool to Identify at Risk Patients who has a chance of becoming users of High-Cost Healthcare service and subsequently Reducing PMPM (Per Member Per Month) Costs While Increasing Member Satisfaction
Weitzman 2013: State Health Policy Initiatives as Drivers for Improving Care...CHC Connecticut
Sue Birch presents on State Health Policy Initiatives as Drivers for Improving Care Outcomes: Colorado's Accountable Care Collaborative at the 2013 Weitzman Symposium
March 02, 2018
Value-based health care is one of the most pressing topics in health care finance and policy today. Value-based payment structures are widely touted as critical to controlling runaway health care costs, but are often difficult for health care entities to incorporate into their existing infrastructures. Because value-based health care initiatives have bipartisan support, it is likely that these programs will continue to play a major role in both the public and private health insurance systems. As such, there is a pressing need to evaluate the implementation of these initiatives thus far and to discuss the direction that American health care financing will take in the coming years.
To explore this important issue, the Petrie-Flom Center for Health Law Policy, Biotechnology, and Bioethics at Harvard Law School collaborated with Ropes & Gray LLP to host a one-day conference on value-based health care. This event brought together scholars, health law practitioners, and health care entities to evaluate the impact of value-based health care on the American health care system.
For more information, visit our website at: http://petrieflom.law.harvard.edu/events/details/will-value-based-care-save-the-health-care-system
Soraya Ghebleh - Unwarranted Variation in HealthcareSoraya Ghebleh
This is a short paper by Soraya Ghebleh that discusses the causes of unwarranted variation in healthcare delivery and potential strategies to reduce these unwarranted variations.
Anti-cancer therapy is big business. In Australia alone between 2000 and 2009, cancer-related pharmaceutical expenditure has risen over 200% to over half a billion dollars per annum.
NVTC Capital Health Tech Summit: Dr. Shannon KeynoteAlexa Magdalenski
The 2017 Capital Health Tech Summit took place on June 15, 2017 at the Inova Center for Personalized Health. Dr. Richard Shannon, Executive Vice President, Health Affairs, University of Virginia provided the Summit's second keynote.
Transforming Medicine Through Personalized Health Care at Ohio State Universi...Ryan Squire
Dr. Clay Marsh presented "Transforming Medicine Through Personalized Health Care at Ohio State University Medical Center" at the 2009 Personalized Health Care National Conference.
Dr. Marsh is leading the Ohio State University Center for Personalized Health Care to create the future of medicine to improve people’s lives through personalized health care.
Implementing a shared care model to prevent liver cancer and improve chronic ...Cancer Institute NSW
Hepatocellular cancer (HCC) is among the top 10 causes of cancer death in Australia, with ~80% of cases attributable to chronic viral hepatitis. Although 60-80% of HCCs are preventable by antiviral therapies, multiple barriers exist in the diagnostic and treatment continuum. Chronic hepatitis B (CHB) is the main cause for rising HCC rates in Western Sydney, where the greatest burden of disease is among people born in hepatitis B endemic countries.
The Affordable Care Act of 2010 (ACA) opens the door to a wealth of opportunities for hospitals and physician groups. They are beginning to adapt to the new pay-for-performance and bundled payment systems and develop population-based care management programs. While the goal of ACA is to hold hospitals and physicians jointly responsible for quality and cost of care, the new payment models span the entire care continuum, including primary care physicians (PCPs), specialists, hospitals, post-acute care, and re-admissions. The biggest winners will be those who can improve quality of care while driving down costs. Those that focus first on preventive care for top chronic illnesses will be the first to cross the finish line.
Soraya Ghebleh - Unwarranted Variation in HealthcareSoraya Ghebleh
This is a short paper by Soraya Ghebleh that discusses the causes of unwarranted variation in healthcare delivery and potential strategies to reduce these unwarranted variations.
Anti-cancer therapy is big business. In Australia alone between 2000 and 2009, cancer-related pharmaceutical expenditure has risen over 200% to over half a billion dollars per annum.
NVTC Capital Health Tech Summit: Dr. Shannon KeynoteAlexa Magdalenski
The 2017 Capital Health Tech Summit took place on June 15, 2017 at the Inova Center for Personalized Health. Dr. Richard Shannon, Executive Vice President, Health Affairs, University of Virginia provided the Summit's second keynote.
Transforming Medicine Through Personalized Health Care at Ohio State Universi...Ryan Squire
Dr. Clay Marsh presented "Transforming Medicine Through Personalized Health Care at Ohio State University Medical Center" at the 2009 Personalized Health Care National Conference.
Dr. Marsh is leading the Ohio State University Center for Personalized Health Care to create the future of medicine to improve people’s lives through personalized health care.
Implementing a shared care model to prevent liver cancer and improve chronic ...Cancer Institute NSW
Hepatocellular cancer (HCC) is among the top 10 causes of cancer death in Australia, with ~80% of cases attributable to chronic viral hepatitis. Although 60-80% of HCCs are preventable by antiviral therapies, multiple barriers exist in the diagnostic and treatment continuum. Chronic hepatitis B (CHB) is the main cause for rising HCC rates in Western Sydney, where the greatest burden of disease is among people born in hepatitis B endemic countries.
The Affordable Care Act of 2010 (ACA) opens the door to a wealth of opportunities for hospitals and physician groups. They are beginning to adapt to the new pay-for-performance and bundled payment systems and develop population-based care management programs. While the goal of ACA is to hold hospitals and physicians jointly responsible for quality and cost of care, the new payment models span the entire care continuum, including primary care physicians (PCPs), specialists, hospitals, post-acute care, and re-admissions. The biggest winners will be those who can improve quality of care while driving down costs. Those that focus first on preventive care for top chronic illnesses will be the first to cross the finish line.
Patient Centered Medical home talk at WVUPaul Grundy
To employers the cost of healthcare is now a business issue and this talk is about what one large buyer IBM did to drive transformation via broad coalition with other large employers to form the Patient Centered Medical Home movement and the covenant between buyer and provider away from the garbage we now buy episodic uncoordinated disintegrated care. In the change of convenient conversation we have worked with the Primary care providers to give us coordinated, integrated, accessible and compressive care with a set of principles know as the Patient centered medical home.
A Patient Centered Medical Home (PCMH) happens when primary care healers keeping that core healing relationship with their patients step up to become specialists in Family and Community Medicine. The move is to the discipline of leading a team that delivers population health management, patent centered prevention, care that is coordination, comprehensive accessible 24/7 and integrated across a deliver system. PCMH happens when the specialists in Family and Community Medicine wake up every morning and ask the question how will my team improve the health of my community today?
All over the world three huge factors are in play that is driving the concept of Patient Centered Medical Home. They are:
1) Cost and demography
2) Information technology and data (information that is actionable will equal a demand for accountability by the payer or buyer of the care)
3) Consumer demand to engage healthcare differently (at least as well as they can their bank- on line) have a question about lab results why not e-mail?
But at its core it is a move toward integration of a healing relationship in primary care and population management all at the point of care with the tools to do just that.
Edwina Rogers, executive director of Patient-Centered Primary Care Collaborative, began her presentation by highlighting the movement to advance medical homes.
With the U.S. being the number one in the world for the cost of healthcare and ranked number 37 in the quality category, something needs to change. Rogers discussed the broad stakeholder support and participation for the movement, as well as the incredible volunteer involvement. The four ‘centers’ include: the Center to Promote Public-Payer Implementation, the Center for Multi-Stakeholder Demonstration, the Center for eHealth Information Adoption and Exchange and the Center for Health Benefit Redesign and Implementation. Medical Homes will provide superb access to care, patient engagament in care, clinical information systems, care coordination, team care, patient feedback and publically available information.
Edwards explained that the Obama administration believes the medical homes concept is the best way to approach healthcare reform. The U.S. House of Representatives has showed great support for the movement and is helping develop and allocate funds for a five-year pilot program. She expressed her enthusiasm for the movement and her prediction that the medical home model is certainly the future of health care.
A complete version of Rogers’ presentation on the Patient-Centered Primary Care Collaborative is available online.
Population Health Management & Volume To Value Based CareIFAH
A session by Amish Purohit, CEO and CMO, US Health Systems on the topic of 'Population Health Management & Volume To Value Based Care' at IFAH USA 2019 held at Caesars Palace, 18-20 June, 2019.
Clinical practice guidelines and quality metrics often emphasize effectiveness over patient-centered care. In this article, the authors offer three approaches to personalizing quality measurement to ensure patient preferences and values guide all clinical decisions.
Clinical practice guidelines and quality metrics often emphasize effectiveness over patient-centered care. In this article, the authors offer three approaches to personalizing quality measurement to ensure patient preferences and values guide all clinical decisions.
How to Engage Physicians in Best Practices to Respond to Healthcare Transform...PYA, P.C.
PYA Principal Kent Bottles, MD, spoke about physician engagement when it comes to value payment models during “How to Engage Physicians in Best Practices to Respond to Healthcare Transformation” at the Georgia Society of Certified Public Accountants’ (GSCPA) 2016 Healthcare Conference, February 11, 2016. Dr. Bottles discussed the difficulty of weaning physicians from fee-for-service payment models and the often-unappreciated reasoning behind the shift to value-based payment models. He also highlighted MACRA, MIPS, patient satisfaction surveys, Physician Compare, and the ProPublica Surgeon Scorecard.
Population health management real time state-of-health analysispscisolutions
To lower health costs, physician networks and medical homes must employ a closed loop population management program that focus on patient SOH stratification, chronic disease management, care coordination and incentive management. This approach will enable them to consistently reduce ER and inpatient admissions, which are the greatest expenditures in health care today.
The Patient-Centered Medical Home Impact on Cost and Quality: An Annual Revie...CHC Connecticut
Dr. Nwando Olayiwola, Associate Director, Center for Excellence in Primary Care, Assistant Professor, University of California, San Francisco addresses the 2014 Weitzman Symposium on The Patient-Centered Medical Home Impact on Cost and Quality: An Annual Review of Evidence
BPS DCP SIGOPAC Good Practice Guidance in Demonstrating Quality and Outcomes ...Alex King
This report outlines a rigorous, multidimensional framework for evaluating quality and outcomes in psycho-oncology services, which can be flexibly adapted to local needs and priorities.
It aims to challenge psycho-oncology services to develop and standardise procedures that address the clinical and operational aspects of quality, while maintaining a firm focus on the experiential.
The proposed framework focuses on six key domains of service quality:
- Is this service safe?
- Is this service equitable, while also focused on those most in need?
- Is this service timely and responsive?
- Is this service respectful, collaborative and patient-centred?
- Is this service offering effective interventions?
- Is this service contributing to efficient multidisciplinary care?
To address these domains, psycho-oncology services need to draw on multiple, convergent sources of data, including key performance indicators, activity levels, patient self-report measures, feedback from professional colleagues, etc.
Patient-centered medical homes (PCMHs) are intended to actively provide effective care by physician-led teams, Where patients take a leading role and responsibility. Objective: To determine whether the Walter Reed PCMH has reduced costs while at least maintaining if not improving access to and quality of care, and to determine
whether access, quality, and cost impacts differ by chronic condition status. Design, setting, and patients: This study
conducted a retrospective analysis using a patient-level utilization database to determine the impact of the Walter Reed PCMH on utilization and cost metrics, and a survey of enrollees in the Walter Reed PCMH to address access to care and quality of care. Outcome measures: Inpatient and outpatient utilization, per member per quarter costs, Healthcare Effectiveness Data and Information Set metrics, and composite measures for access, patient satisfaction, provider communication, and customer service are included. Results: Costs were 11% lower for those with chronic conditions compared to 7% lower for those without. Since treating patients with chronic conditions is 4 times more costly than treating patients without such conditions, the vast majority of dollar savings are attributable to chronic care.
Running Head Colorectal Cancer Prevention Program-Evaluation Des.docxaryan532920
Running Head: Colorectal Cancer Prevention Program-Evaluation Design 9
Colorectal Cancer Prevention Program Evaluation Design
Kaplan University-PU630-Unit 7
September 20, 2016
Deserie Thomas
Dr. Amy Thompson
COLORECTAL CANCER PREVENTION PROGRAM EVALUATION DESIGN
Engaged Stakeholders What Stakeholders Want to Know
Public Health Department
Document the resources that have been leveraged to support colorectal cancer prevention program efforts.
Local Legislators
Identify the number of people receiving services and the extent to which interventions are yielding intended awareness, behavioral and/or health outcomes for participants.
Intervention participants
Determine the extent to which interventions are yielding intended awareness, behavioral and/or health outcomes for participants.
Community Clinic
Review the quality, contributions, and impact of the Colorectal Cancer Coalition.
Review the quality and implementation progress of the statewide Colorectal Cancer Coalition plan.
Determine to what extent interventions outlined in the Colorectal Cancer Coalition action plan are being executed and yielding intended results.
Local American Cancer Society Partner
Determine whether American Cancer Society products are being incorporated effectively into the efforts of the colorectal cancer prevention program.
Engaging Stakeholders
Health Department
Members of the evaluation advisory committee
Presenters/advocates who share findings with state and community partners
All phases of the evaluation process via regular evaluation advisory committee meetings
Legislators
External reviewers of evaluation plans and methods
Evaluation planning phase
Intervention Participants
Members of the evaluation advisory committee
Data sources (i.e., participants in evaluation interviews and surveys)
Two representatives to participate in all phases of the evaluation process via regular evaluation advisory committee
Community Clinic
External reviewers of evaluation plans and methods
Evaluation implementation phase
Evaluation planning phase
Local American Cancer Society Partner
Data analysts Presenters/advocates who share findings with state and community partners
Evaluation implementation phase Dissemination phase
Evaluation Stakeholder Group Composition
The composition of the evaluation stakeholders will fund and authorized the continuation or expansion of the Colorectal Cancer Prevention Program. The stakeholders are responsible for day to day implementation of the activities that are part of the program, and has a strong influence on the development of thoughtful evaluation questions that will generate evaluation findings that are useful, relevant, and credible (assuming the evaluation applies the appropriate design and data collection and analysis methods). Ideally, the evaluation stakeholders gro ...
Team as Treatment: Driving Improvement in DiabetesCHC Connecticut
NCA Clinical Workforce Development, Team-Based Care 2019 Webinar Series
Webinar broadcast on: June 11, 2019 | 3 p.m. EST
This webinar will share evidence-based models that will provide a framework for health centers to optimize the team in primary care. Experts will describe how utilization of extended team members and technology can reduce gaps in care for prediabetics and diabetics. With a focus on lifestyle and community based projects, this webinar will highlight the strategies and resources to improve the health and behaviors of patients at risk for diabetes and manage uncontrolled diabetes. Through early detection and providing diabetes management through a team-based care, health centers can help patients’ live long, healthy lives.
1. Lynn A. Godfrey, MPH Candidate – May 2016 │ Brian Martin, Ph.D., Academic Advisor| EVMS Helena Deligt, LCSW – COO, Programs│ Daily Planet, FQHC, Richmond, VA
Introduction
In 2007, the American Academy of Pediatrics (AAP), American
College of Physicians (ACP), American Academy of Family
Physicians (AAFP), and the American Osteopathic Academy
(AOA) came together to issue their influential “Joint Principles of
the Patient-Centered Medical Home (PCMH).” The PCMH is an
innovative model of care characterized by comprehensive primary
care, quality improvement, care management, and enhanced
access in a patient-centered environment.
The Daily Planet Healthcare Center is an FQHC practice located in
urban Richmond, VA. It is a primary care clinic which focuses on
serving high-risk patients and underserved and uninsured
populations experiencing homelessness or at-risk of
homelessness. The Clinic was recognized as a level 3 (the
highest) PCMH facility the first year of recognition, 2013: and,
currently is planning for their 2016 recognition renewal.
This study evaluates the Center in quality and costs performances
measures from 2012 – 2014.
Methods
Design
Quality and cost improvement case study utilizing data from the US
Health and Human Services HRSA’s Uniform Data System (UDS).
Data from grantees collected monthly from performance reports
entered in HRSA’s UDS.
Clinical Quality Data
From 2012 to 2014, Daily Planet reported data on a monthly basis to
US HHS, HRSA UDS on six (6) clinical quality measures of prevention
and chronic disease management. The measures are:
Preventive Health Screening and Services: Weight screening – adults
and adolescents; Tobacco use; colorectal cancer; cervical cancer; and,
depression screening.
Chronic Disease Management: Asthma treatment; cholesterol treatment;
heart attach/stroke; blood pressure treatment; diabetes control; and, HIV
linkage.
Cost Data
Comparative cost data measuring total cost per patient and total cost
per visit from 2012 -2014 for the health center, the state in which it
operates, and nationally.
Analyses
Adjusted quartile rankings provides the health center’s quartile
ranking compared to health centers nationally for each of the clinical
performance measures. Clinical performance for each measure is
ranked from quartile 1 (highest 25% of reporting health centers) to
quartile 4 (lowest 25% of reporting health centers).
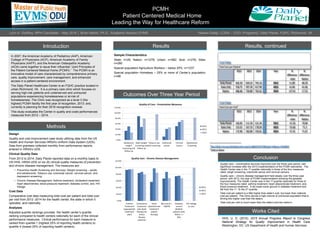
Results
Outcomes Over Three Year Period
Results, continued
Cost Data
Total Cost per Patienti
2012 2013 2014 Year %
difference
- state
%
difference
- Nation
Daily Planet 602.39 659.23 745.10 2012 51.89 -84.29
State (VA) 550.75 597.39 617.99 2013 61.84 -61.66
Nation 686.68 720.89 762.62 2014 127.41 -17.52
Cost Data
Total Cost per Visitii
2012 2013 2014 Year %
difference
- state
%
difference
- Nation
Daily Planet 102.05 111.59 121.34 2012 -51.50 -70.94
State (VA) 153.55 167.19 178.59 2013 -55.60 -71.3
Nation 172.99 182.89 193.01 2014 -57.25 -71.67
i
http://bphc.hrsa.gov/uds/datacenter.aspx?q=d&bid=031720&state=VA&year=2014#fn6
ii
Same as above
Conclusion
• Quality care – preventative services improved over the three year period, with
significant increase after the 2013 implementation of the PCMH standards. The
Health Center was in the 1st quartile nationally in three of the four measures
rated: weigh screening; colorectal cancer and cervical cancers.
• Quality care – chronic disease management held steady over the three year
period, with 2013, the year of PCMH implementation showing the greatest
improvements. The Health Center was in the 1st quartile nationally for three of
the four measures rated: asthma treatment; heart attack/stroke treatment; and,
blood pressure treatment. It did loose some ground in diabetes treatment and
fell from the 1st. To the 3rd quartile.
• Total cost per patient is a little higher than state’s cost, but lower than national
cost per patient. The Clinic serves a high volume of uninsured population that is
driving this higher cost than the state’s.
• Total cost per visit is much lower than the state’s and the nation’s.
Works Cited
• HHS, U. D. (2015). 2015 Annual Progress Report to Congress:
National Strategy for Quality Improvement in Health Care.
Washington, DC: US Department of Health and Human Services.
PCMH
pPatient Centered Medical Home
Leading the Way for Healthcare Reform
Sample Characteristics
State: n=26; Nation: n=1278; Urban: n=582; Size: n=276; Sites:
n=280
Special population Agriculture Workers – below 25%: n=1237
Special population Homeless – 25% or more of Center’s population:
n=88
0.00%
20.00%
40.00%
60.00%
80.00%
100.00%
120.00%
Adolescent
weight
screening and
follow-up
Adult weight
screening and
follow-up
Tobacco use
and screening
Colorectal
cancer
Cervical
Cancer
Depresssion
Screening
Quality of Care - Preventative Measures
2012
2013
2014
0.00%
20.00%
40.00%
60.00%
80.00%
100.00%
120.00%
Asthma
Treatment
(appropriate
treatment
plan)
Cholesterol
treatment
plan (lipid
therapy for
artery
disease
patients)
Heart
attack/stroke
treatment
(aspirin
therapy)
Bp control <
140/90
Diabetes
control
(diabetic
patients with
HbA1c <=
9%)
HIV linkage
to care
Quality Care - Chronic Disease Management
2012
2013
2014