Download to read offline
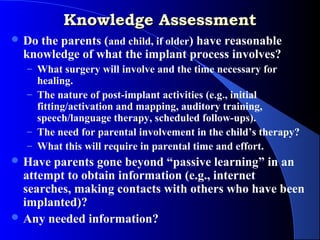




This document discusses issues related to behavior management for children receiving cochlear implants. It begins by outlining topics covered in pre-implant psychological evaluations, such as family support and expectations. These evaluations help identify children who may benefit from intervention to address behavioral challenges. The document then describes two common childhood disorders, oppositional defiant disorder and ADHD, that can impact success. Finally, it overviews behavioral treatment approaches like modeling, reinforcement, and punishment that can help manage behaviors and facilitate positive implant outcomes.





















































