Downloaded 48 times
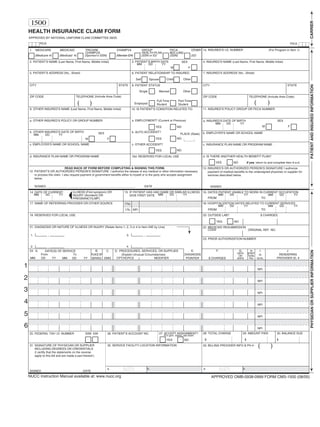

This document is a health insurance claim form containing sections for inputting patient and insured information, physician/supplier information, diagnosis codes, procedures, dates of service, charges and billing amounts. It includes fields for identifying the patient, their insurance plan and relationship to the insured. Sections are also included for provider details, diagnoses, services rendered, charges and required signatures. The form is used to submit medical claims to health insurance plans for reimbursement.