Daily maintenance sheet
•A daily medical lab maintenance sheet covers
general cleanliness, equipment checks, PPE/Safety
, consumables, and waste management, focusing
on daily tasks like wiping benches, restocking
soap/towels, checking emergency stations, cleaning
key equipment exteriors, and proper
glassware/waste disposal, all to prevent
contamination and ensure accuracy, referencing
equipment manuals for specifics.
15.
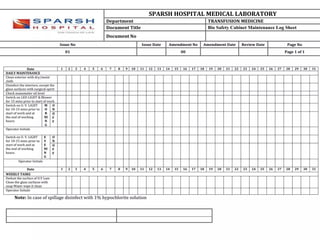
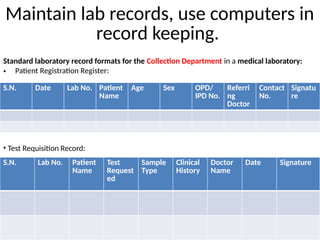
Maintain lab records,use computers in
record keeping.
Standard laboratory record formats for the Collection Department in a medical laboratory:
• Patient Registration Register:
S.N. Date Lab No. Patient
Name
Age Sex OPD/
IPD No.
Referri
ng
Doctor
Contact
No.
Signatu
re
• Test Requisition Record:
S.N. Lab No. Patient
Name
Test
Request
ed
Sample
Type
Clinical
History
Doctor
Name
Date Signature
16.
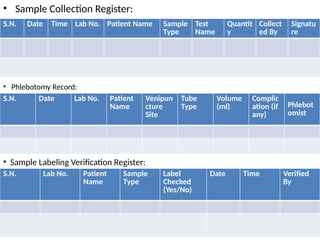
• Sample CollectionRegister:
S.N. Date Time Lab No. Patient Name Sample
Type
Test
Name
Quantit
y
Collect
ed By
Signatu
re
• Phlebotomy Record:
S.N. Date Lab No. Patient
Name
Venipun
cture
Site
Tube
Type
Volume
(ml)
Complic
ation (if
any)
Phlebot
omist
• Sample Labeling Verification Register:
S.N. Lab No. Patient
Name
Sample
Type
Label
Checked
(Yes/No)
Date Time Verified
By
17.
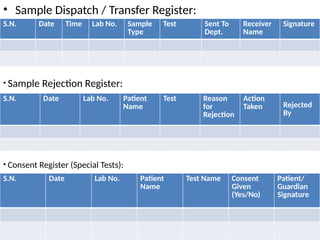
• Sample Dispatch/ Transfer Register:
S.N. Date Time Lab No. Sample
Type
Test Sent To
Dept.
Receiver
Name
Signature
• Sample Rejection Register:
S.N. Date Lab No. Patient
Name
Test Reason
for
Rejection
Action
Taken Rejected
By
• Consent Register (Special Tests):
S.N. Date Lab No. Patient
Name
Test Name Consent
Given
(Yes/No)
Patient/
Guardian
Signature
18.
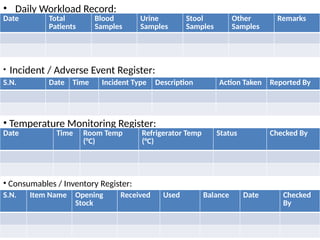
• Daily WorkloadRecord:
Date Total
Patients
Blood
Samples
Urine
Samples
Stool
Samples
Other
Samples
Remarks
• Incident / Adverse Event Register:
S.N. Date Time Incident Type Description Action Taken Reported By
• Temperature Monitoring Register:
Date Time Room Temp
(°C)
Refrigerator Temp
(°C)
Status Checked By
• Consumables / Inventory Register:
S.N. Item Name Opening
Stock
Received Used Balance Date Checked
By
19.
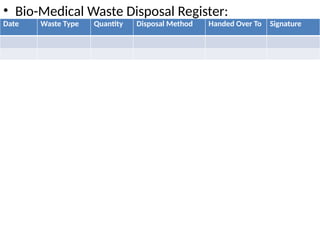
• Bio-Medical WasteDisposal Register:
Date Waste Type Quantity Disposal Method Handed Over To Signature
20.
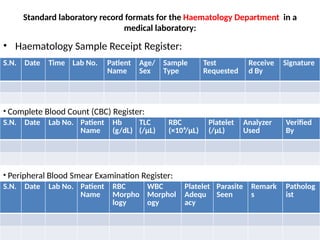
Standard laboratory recordformats for the Haematology Department in a
medical laboratory:
• Haematology Sample Receipt Register:
S.N. Date Time Lab No. Patient
Name
Age/
Sex
Sample
Type
Test
Requested
Receive
d By
Signature
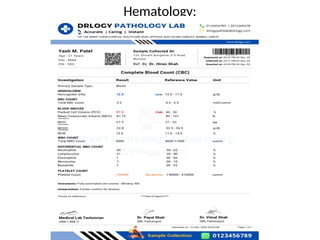
• Complete Blood Count (CBC) Register:
S.N. Date Lab No. Patient
Name
Hb
(g/dL)
TLC
(/µL)
RBC
(×10⁶/µL)
Platelet
(/µL)
Analyzer
Used
Verified
By
• Peripheral Blood Smear Examination Register:
S.N. Date Lab No. Patient
Name
RBC
Morpho
logy
WBC
Morphol
ogy
Platelet
Adequ
acy
Parasite
Seen
Remark
s
Patholog
ist
21.
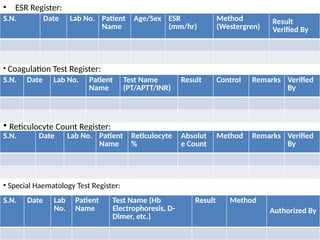
• ESR Register:
S.N.Date Lab No. Patient
Name
Age/Sex ESR
(mm/hr)
Method
(Westergren)
Result
Verified By
• Coagulation Test Register:
S.N. Date Lab No. Patient
Name
Test Name
(PT/APTT/INR)
Result Control Remarks Verified
By
• Reticulocyte Count Register:
S.N. Date Lab No. Patient
Name
Reticulocyte
%
Absolut
e Count
Method Remarks Verified
By
• Special Haematology Test Register:
S.N. Date Lab
No.
Patient
Name
Test Name (Hb
Electrophoresis, D-
Dimer, etc.)
Result Method
Authorized By
22.
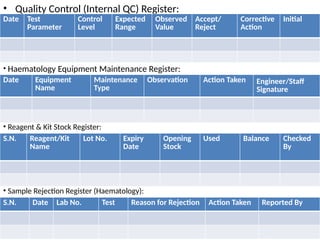
• Quality Control(Internal QC) Register:
Date Test
Parameter
Control
Level
Expected
Range
Observed
Value
Accept/
Reject
Corrective
Action
Initial
• Haematology Equipment Maintenance Register:
Date Equipment
Name
Maintenance
Type
Observation Action Taken Engineer/Staff
Signature
• Reagent & Kit Stock Register:
S.N. Reagent/Kit
Name
Lot No. Expiry
Date
Opening
Stock
Used Balance Checked
By
• Sample Rejection Register (Haematology):
S.N. Date Lab No. Test Reason for Rejection Action Taken Reported By
23.
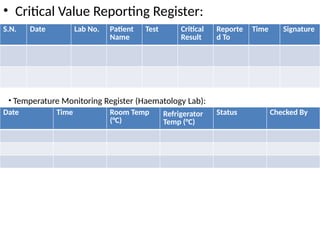
• Critical ValueReporting Register:
S.N. Date Lab No. Patient
Name
Test Critical
Result
Reporte
d To
Time Signature
• Temperature Monitoring Register (Haematology Lab):
Date Time Room Temp
(°C)
Refrigerator
Temp (°C)
Status Checked By
24.
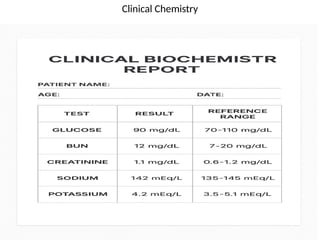
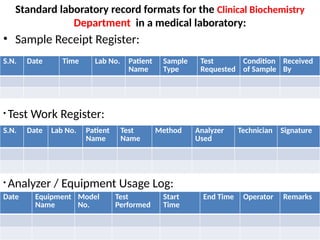
Standard laboratory recordformats for the Clinical Biochemistry
Department in a medical laboratory:
• Sample Receipt Register:
S.N. Date Time Lab No. Patient
Name
Sample
Type
Test
Requested
Condition
of Sample
Received
By
• Test Work Register:
S.N. Date Lab No. Patient
Name
Test
Name
Method Analyzer
Used
Technician Signature
• Analyzer / Equipment Usage Log:
Date Equipment
Name
Model
No.
Test
Performed
Start
Time
End Time Operator Remarks
25.
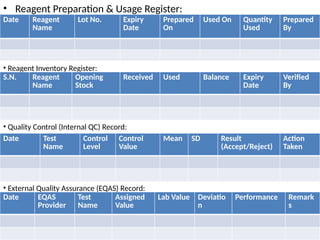
• Reagent Preparation& Usage Register:
Date Reagent
Name
Lot No. Expiry
Date
Prepared
On
Used On Quantity
Used
Prepared
By
• Reagent Inventory Register:
S.N. Reagent
Name
Opening
Stock
Received Used Balance Expiry
Date
Verified
By
• Quality Control (Internal QC) Record:
Date Test
Name
Control
Level
Control
Value
Mean SD Result
(Accept/Reject)
Action
Taken
• External Quality Assurance (EQAS) Record:
Date EQAS
Provider
Test
Name
Assigned
Value
Lab Value Deviatio
n
Performance Remark
s
26.
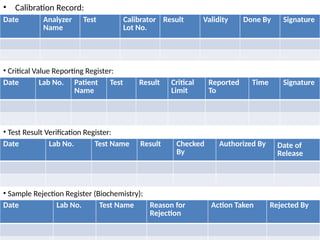
• Calibration Record:
DateAnalyzer
Name
Test Calibrator
Lot No.
Result Validity Done By Signature
• Critical Value Reporting Register:
Date Lab No. Patient
Name
Test Result Critical
Limit
Reported
To
Time Signature
• Test Result Verification Register:
Date Lab No. Test Name Result Checked
By
Authorized By Date of
Release
• Sample Rejection Register (Biochemistry):
Date Lab No. Test Name Reason for
Rejection
Action Taken Rejected By
27.
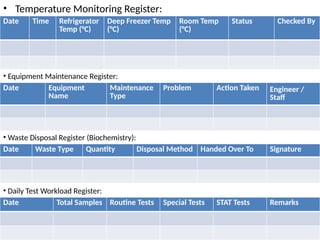
• Temperature MonitoringRegister:
Date Time Refrigerator
Temp (°C)
Deep Freezer Temp
(°C)
Room Temp
(°C)
Status Checked By
• Equipment Maintenance Register:
Date Equipment
Name
Maintenance
Type
Problem Action Taken Engineer /
Staff
• Waste Disposal Register (Biochemistry):
Date Waste Type Quantity Disposal Method Handed Over To Signature
• Daily Test Workload Register:
Date Total Samples Routine Tests Special Tests STAT Tests Remarks
28.
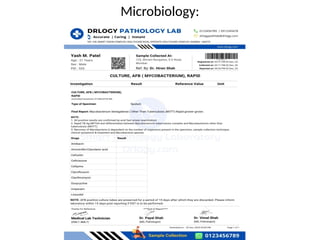
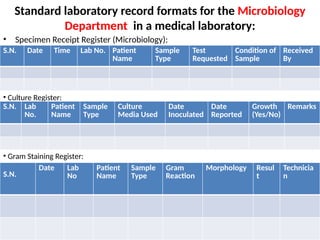
Standard laboratory recordformats for the Microbiology
Department in a medical laboratory:
• Specimen Receipt Register (Microbiology):
S.N. Date Time Lab No. Patient
Name
Sample
Type
Test
Requested
Condition of
Sample
Received
By
• Culture Register:
S.N. Lab
No.
Patient
Name
Sample
Type
Culture
Media Used
Date
Inoculated
Date
Reported
Growth
(Yes/No)
Remarks
• Gram Staining Register:
S.N.
Date Lab
No
Patient
Name
Sample
Type
Gram
Reaction
Morphology Resul
t
Technicia
n
29.
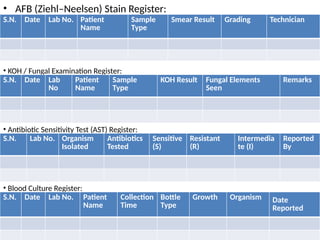
• AFB (Ziehl–Neelsen)Stain Register:
S.N. Date Lab No. Patient
Name
Sample
Type
Smear Result Grading Technician
• KOH / Fungal Examination Register:
S.N. Date Lab
No
Patient
Name
Sample
Type
KOH Result Fungal Elements
Seen
Remarks
• Antibiotic Sensitivity Test (AST) Register:
S.N. Lab No. Organism
Isolated
Antibiotics
Tested
Sensitive
(S)
Resistant
(R)
Intermedia
te (I)
Reported
By
• Blood Culture Register:
S.N. Date Lab No. Patient
Name
Collection
Time
Bottle
Type
Growth Organism Date
Reported
30.
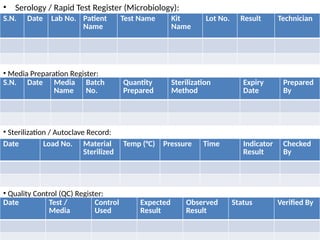
• Serology /Rapid Test Register (Microbiology):
S.N. Date Lab No. Patient
Name
Test Name Kit
Name
Lot No. Result Technician
• Media Preparation Register:
S.N. Date Media
Name
Batch
No.
Quantity
Prepared
Sterilization
Method
Expiry
Date
Prepared
By
• Sterilization / Autoclave Record:
Date Load No. Material
Sterilized
Temp (°C) Pressure Time Indicator
Result
Checked
By
• Quality Control (QC) Register:
Date Test /
Media
Control
Used
Expected
Result
Observed
Result
Status Verified By
31.
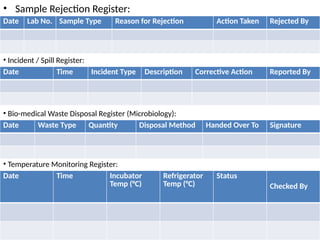
• Sample RejectionRegister:
Date Lab No. Sample Type Reason for Rejection Action Taken Rejected By
• Incident / Spill Register:
Date Time Incident Type Description Corrective Action Reported By
• Bio-medical Waste Disposal Register (Microbiology):
Date Waste Type Quantity Disposal Method Handed Over To Signature
• Temperature Monitoring Register:
Date Time Incubator
Temp (°C)
Refrigerator
Temp (°C)
Status
Checked By
32.
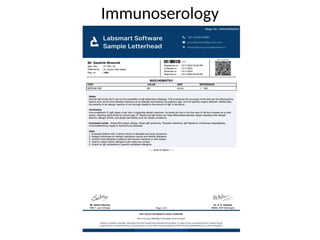
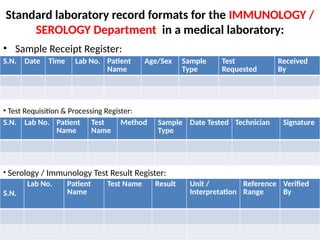
Standard laboratory recordformats for the IMMUNOLOGY /
SEROLOGY Department in a medical laboratory:
• Sample Receipt Register:
S.N. Date Time Lab No. Patient
Name
Age/Sex Sample
Type
Test
Requested
Received
By
• Test Requisition & Processing Register:
S.N. Lab No. Patient
Name
Test
Name
Method Sample
Type
Date Tested Technician Signature
• Serology / Immunology Test Result Register:
S.N.
Lab No. Patient
Name
Test Name Result Unit /
Interpretation
Reference
Range
Verified
By
33.
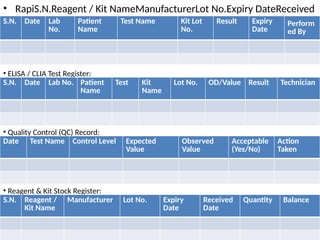
• RapiS.N.Reagent /Kit NameManufacturerLot No.Expiry DateReceived
DateQuantityBalanced Test Register (HIV, HBsAg, HCV, Dengue,
Malaria, etc.)
S.N. Date Lab
No.
Patient
Name
Test Name Kit Lot
No.
Result Expiry
Date
Perform
ed By
• ELISA / CLIA Test Register:
S.N. Date Lab No. Patient
Name
Test Kit
Name
Lot No. OD/Value Result Technician
• Quality Control (QC) Record:
Date Test Name Control Level Expected
Value
Observed
Value
Acceptable
(Yes/No)
Action
Taken
• Reagent & Kit Stock Register:
S.N. Reagent /
Kit Name
Manufacturer Lot No. Expiry
Date
Received
Date
Quantity Balance
34.
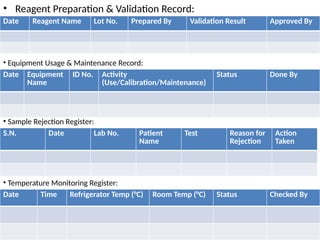
• Reagent Preparation& Validation Record:
Date Reagent Name Lot No. Prepared By Validation Result Approved By
• Equipment Usage & Maintenance Record:
Date Equipment
Name
ID No. Activity
(Use/Calibration/Maintenance)
Status Done By
• Sample Rejection Register:
S.N. Date Lab No. Patient
Name
Test Reason for
Rejection
Action
Taken
• Temperature Monitoring Register:
Date Time Refrigerator Temp (°C) Room Temp (°C) Status Checked By
35.
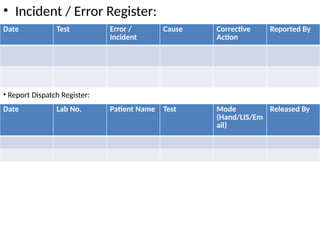
• Incident /Error Register:
Date Test Error /
Incident
Cause Corrective
Action
Reported By
• Report Dispatch Register:
Date Lab No. Patient Name Test Mode
(Hand/LIS/Em
ail)
Released By
36.
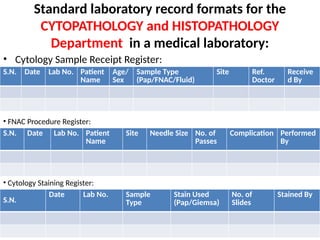
Standard laboratory recordformats for the
CYTOPATHOLOGY and HISTOPATHOLOGY
Department in a medical laboratory:
• Cytology Sample Receipt Register:
• :
S.N. Date Lab No. Patient
Name
Age/
Sex
Sample Type
(Pap/FNAC/Fluid)
Site Ref.
Doctor
Receive
d By
• FNAC Procedure Register:
S.N. Date Lab No. Patient
Name
Site Needle Size No. of
Passes
Complication Performed
By
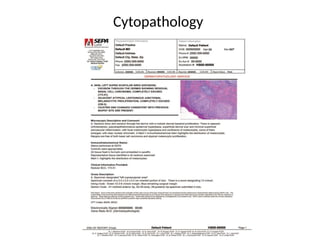
• Cytology Staining Register:
S.N.
Date Lab No. Sample
Type
Stain Used
(Pap/Giemsa)
No. of
Slides
Stained By
37.
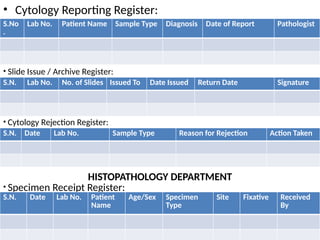
• Cytology ReportingRegister:
S.No
.
Lab No. Patient Name Sample Type Diagnosis Date of Report Pathologist
• Slide Issue / Archive Register:
S.N. Lab No. No. of Slides Issued To Date Issued Return Date Signature
• Cytology Rejection Register:
S.N. Date Lab No. Sample Type Reason for Rejection Action Taken
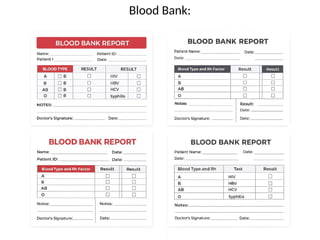
HISTOPATHOLOGY DEPARTMENT
• Specimen Receipt Register:
S.N. Date Lab No. Patient
Name
Age/Sex Specimen
Type
Site Fixative Received
By
38.
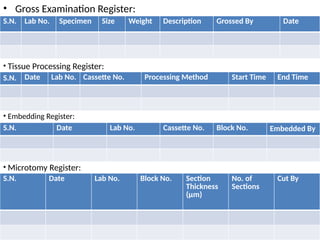
• Gross ExaminationRegister:
S.N. Lab No. Specimen Size Weight Description Grossed By Date
• Tissue Processing Register:
S.N. Date Lab No. Cassette No. Processing Method Start Time End Time
• Embedding Register:
S.N. Date Lab No. Cassette No. Block No. Embedded By
• Microtomy Register:
S.N. Date Lab No. Block No. Section
Thickness
(µm)
No. of
Sections
Cut By
39.
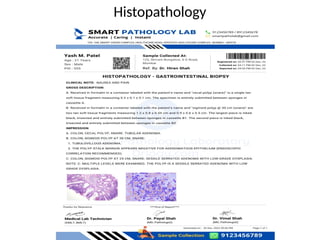
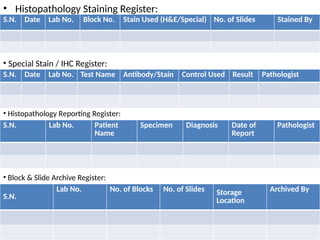
• Histopathology StainingRegister:
S.N. Date Lab No. Block No. Stain Used (H&E/Special) No. of Slides Stained By
• Special Stain / IHC Register:
S.N. Date Lab No. Test Name Antibody/Stain Control Used Result Pathologist
• Histopathology Reporting Register:
S.N. Lab No. Patient
Name
Specimen Diagnosis Date of
Report
Pathologist
• Block & Slide Archive Register:
S.N.
Lab No. No. of Blocks No. of Slides Storage
Location
Archived By
40.
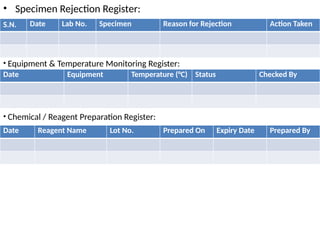
• Specimen RejectionRegister:
S.N. Date Lab No. Specimen Reason for Rejection Action Taken
• Equipment & Temperature Monitoring Register:
Date Equipment Temperature (°C) Status Checked By
• Chemical / Reagent Preparation Register:
Date Reagent Name Lot No. Prepared On Expiry Date Prepared By
41.
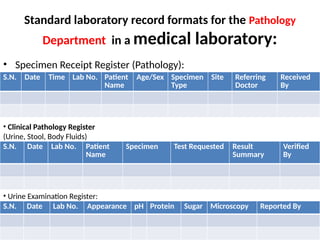
Standard laboratory recordformats for the Pathology
Department in a medical laboratory:
• Specimen Receipt Register (Pathology):
S.N. Date Time Lab No. Patient
Name
Age/Sex Specimen
Type
Site Referring
Doctor
Received
By
• Clinical Pathology Register
(Urine, Stool, Body Fluids)
S.N. Date Lab No. Patient
Name
Specimen Test Requested Result
Summary
Verified
By
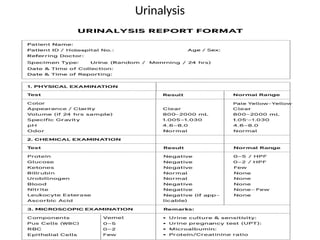
• Urine Examination Register:
S.N. Date Lab No. Appearance pH Protein Sugar Microscopy Reported By
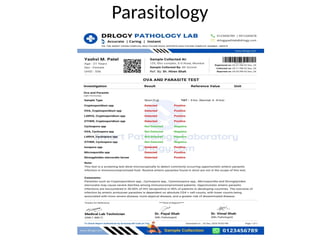
42.
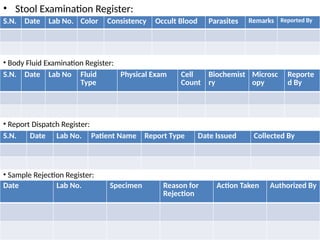
• Stool ExaminationRegister:
S.N. Date Lab No. Color Consistency Occult Blood Parasites Remarks Reported By
• Body Fluid Examination Register:
S.N. Date Lab No Fluid
Type
Physical Exam Cell
Count
Biochemist
ry
Microsc
opy
Reporte
d By
• Report Dispatch Register:
S.N. Date Lab No. Patient Name Report Type Date Issued Collected By
• Sample Rejection Register:
Date Lab No. Specimen Reason for
Rejection
Action Taken Authorized By
43.
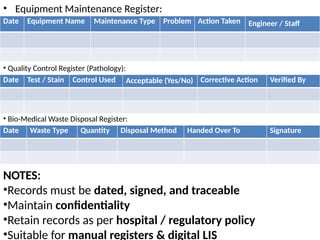
• Equipment MaintenanceRegister:
Date Equipment Name Maintenance Type Problem Action Taken Engineer / Staff
• Quality Control Register (Pathology):
Date Test / Stain Control Used Acceptable (Yes/No) Corrective Action Verified By
• Bio-Medical Waste Disposal Register:
Date Waste Type Quantity Disposal Method Handed Over To Signature
NOTES:
•Records must be dated, signed, and traceable
•Maintain confidentiality
•Retain records as per hospital / regulatory policy
•Suitable for manual registers & digital LIS
44.
Assist to preparecomputerized reports
• To prepare computerized reports for a medical laboratory, we
need a Laboratory Information System (LIS) or Laboratory
Information Management System (LIMS) software.
• These systems automate workflows, manage data, and
generate standardized, accurate reports while ensuring
regulatory compliance.
1. Steps to Prepare Computerized Reports:
• Select a Laboratory Information System (LIS): Choose an LIS
that fits your lab's specific needs, size, and budget. Key
features to look for include:
– Automation: Automatic data transfer from analyzers to the
system reduces manual entry errors.
45.
– Integration: Theability to interface with lab instruments,
Electronic Health Records (EHRs), and billing systems.
– Reporting: Custom report templates, e-signatures for
pathologists, and options for various distribution methods
(print, email, SMS, WhatsApp).
– Compliance: Features that help maintain regulatory
standards like HIPAA (Health Insurance Portability and
Accountability Act), CLIA(Clinical Laboratory
Improvement Amendments), and CAP (College of
American Pathologists ).
2. Standardize Workflows and Templates:
• The LIS software uses pre-configured test details, normal
value ranges (adjustable by age/gender), and
standardized protocols for all procedures.
• This ensures consistency and accuracy in reporting.
46.
3. Implement DataEntry and Tracking:
• Specimen Accessioning: Upon sample collection, the system assigns a unique barcode for
tracking throughout the testing process.
• Test Result Entry: Lab technicians enter test results, which the system can compare to pre-
defined normal values and use for auto-calculations (e.g., for CBC, lipid panels).
4. Generate and Distribute Reports:
– Once results are verified and signed off electronically by a pathologist, the system automatically
generates a complete PDF report.
– Reports often include QR codes for easy patient access and sharing.
– The LIS can automatically send notifications and reports to patients and ordering physicians via
integrated communication channels.
• Standard Report Sections:
A typical computerized medical laboratory report includes:
• Patient Demographics: Name, age, gender, etc.
• Test Details: Name of the test, method used, and instrument info.
• Results: The findings from the analysis, with units and normal reference ranges.
• Interpretation/Discussion: The pathologist's e-signature validates the report, and
interpretations can be included.
• Lab Information: Laboratory's name, contact information, and potentially a letterhead for branding.
• By utilizing a dedicated LIS, laboratories can minimize human error, improve efficiency, and ensure all
data is securely managed and easily accessible for informed clinical decisions.
47.
Maintain lab records,use computers in
record keeping.
• Maintaining lab records, particularly with the use of
computers, involves a combination of established record-
keeping principles and specific digital data management
practices to ensure accuracy, integrity, and traceability.
• General Principles for Lab Record Maintenance:
• Whether records are paper-based, electronic, or a hybrid, core
principles apply:
• Legible, Clear, and Timely: All entries must be made promptly,
using permanent ink for paper or dated/time-stamped entries for
electronic systems.
• Thorough and Complete: Records should be detailed enough that
another person could repeat the experiment or trace a sample's
journey through the lab.
48.
• Accurate andFactual: Avoid opinions or disparaging comments; record
results factually.
• Secure and Organized: Data must be protected from damage, loss, or
unauthorized access and stored in an organized manner for easy
retrieval.
• Signed and Witnessed: Key entries should be signed and dated by the
author and ideally a witness who understands the work but did not
participate in it, especially for legally sensitive work (e.g., patent
applications).
• Using Computers in Record Keeping:
• Computers offer significant benefits like efficiency, easier data analysis,
and enhanced data protection, typically managed through a Laboratory
Information Management System (LIMS), or simpler software like
spreadsheets or databases.
• Practices for Electronic Records:
• Adopt Official Procedures: The lab should have a clear policy on what
constitutes an electronic notebook and how data is managed.
49.
• Using Computersin Record Keeping
• Computers and specialized software (like a Laboratory
Information Management System (LIMS)) streamline
record keeping, replacing manual paperwork and
reducing human error.
• Key Considerations for Electronic Records:
• Software and Tools:
– Simple data can be managed using word processing (e.g.,
Microsoft Word) or spreadsheet software (e.g., Microsoft
Excel).
– For large amounts of complex data, a database management
system or LIMS is recommended, as it allows for better
organization, searching, and analysis.
– Data loggers can automatically collect data from lab
instruments, transferring it directly to a computer.
50.
• Data Securityand Integrity:
– Implement user IDs and passwords or digital signatures to control
access and authenticate users.
– Ensure all data changes are tracked via an audit trail, preserving
the original information and identifying who made the change and
when.
– Store records on unchangeable mediums (WORM - Write Once,
Read Many) or in secure, restricted electronic archives.
• Backup and Retention:
– Establish regular, automated backup systems and store copies in a
secure, distant location to prevent data loss from system failure or
environmental hazards.
– Define a clear retention time for different types of records based
on regulatory requirements (e.g., FDA, ISO standards), contractual
agreements, and the lab's ongoing needs.
– Have a documented process for the eventual deletion or archival of
records once their retention time has expired.
51.
• Best Practices
•Document Processes: Create and follow Standard
Operating Procedures (SOPs) for record management,
including file-naming conventions and folder structures.
• Regular Training: Ensure all staff are trained on the lab's
record-keeping procedures and data management plan.
• Audit Readiness: Design systems so they can be easily
audited by internal quality assurance or external
accreditation bodies to demonstrate compliance.
• Hybrid Systems: If using a mix of paper and electronic
records, maintain clear cross-references between the
two formats and ensure original paper documents are
securely retained.