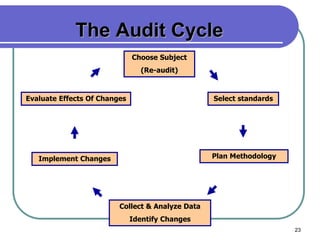
This document provides an overview of how to conduct a clinical audit. It defines clinical audit as a process used by healthcare professionals to systematically review, evaluate and improve patient care. The document outlines the key components of an audit, including choosing a topic, selecting standards, planning methodology, collecting data, analyzing results, and implementing changes. It emphasizes that the goal of audit is to compare current practices to standards in order to enhance quality of care and patient outcomes.