Downloaded 12 times


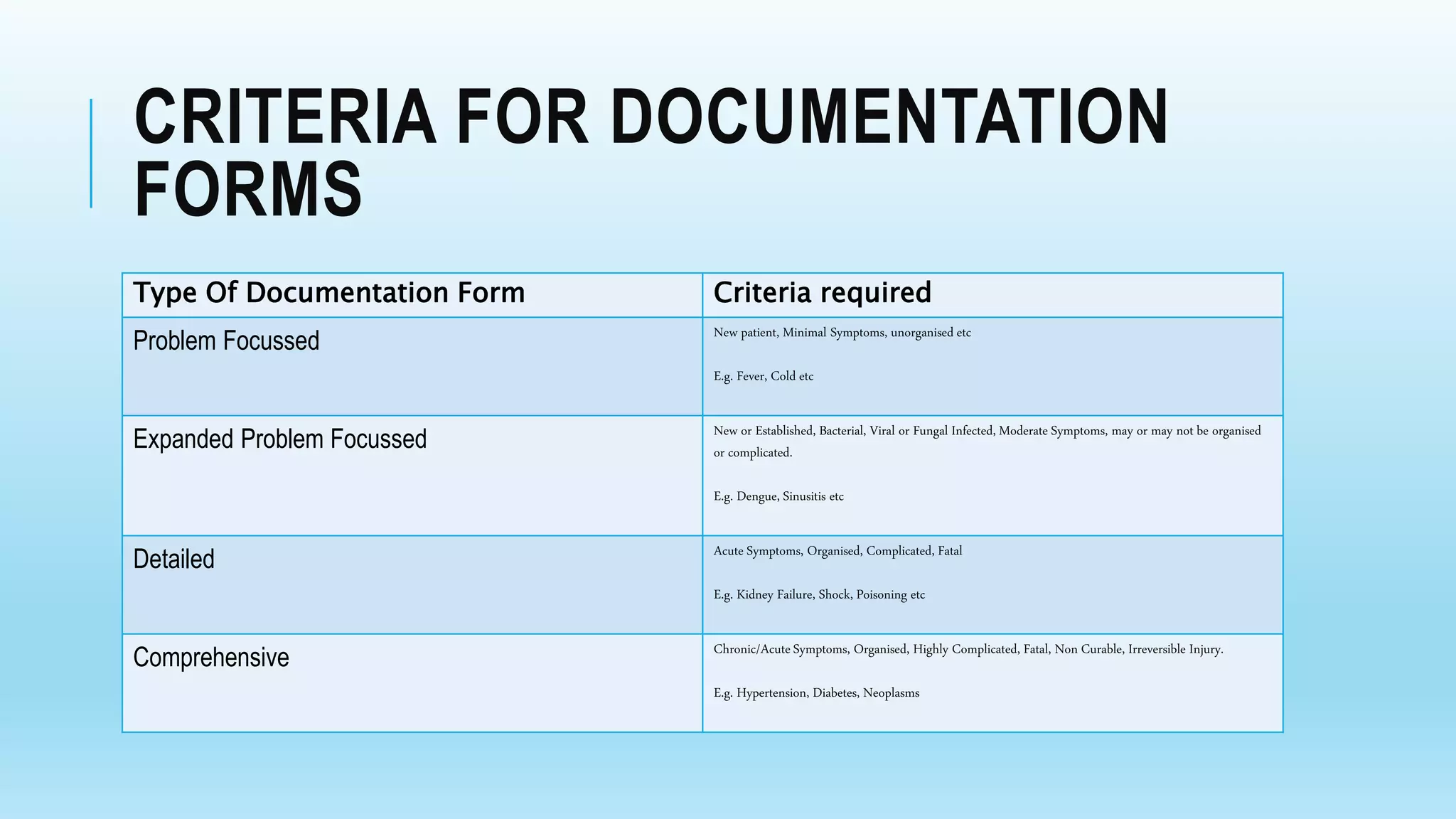




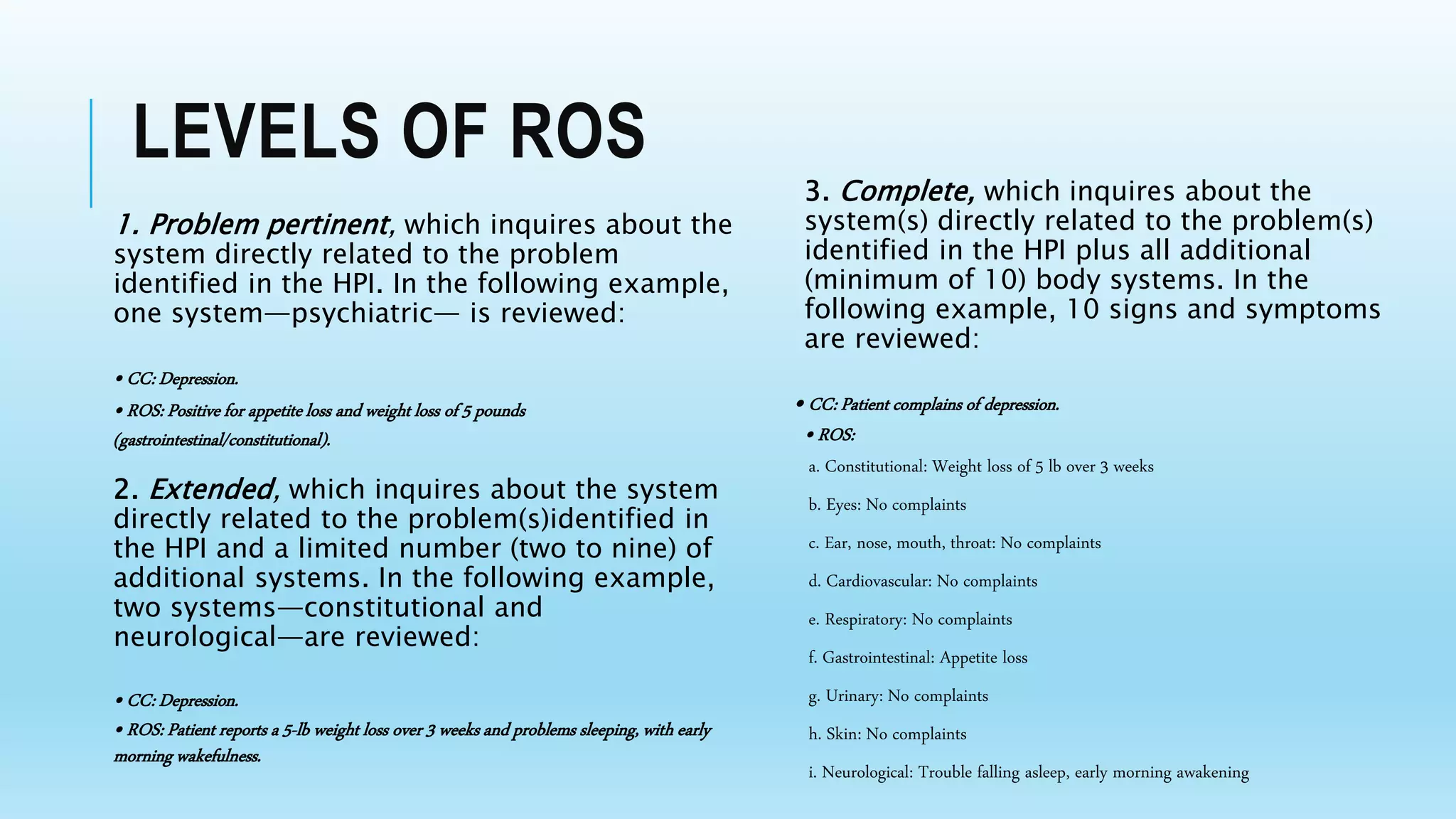



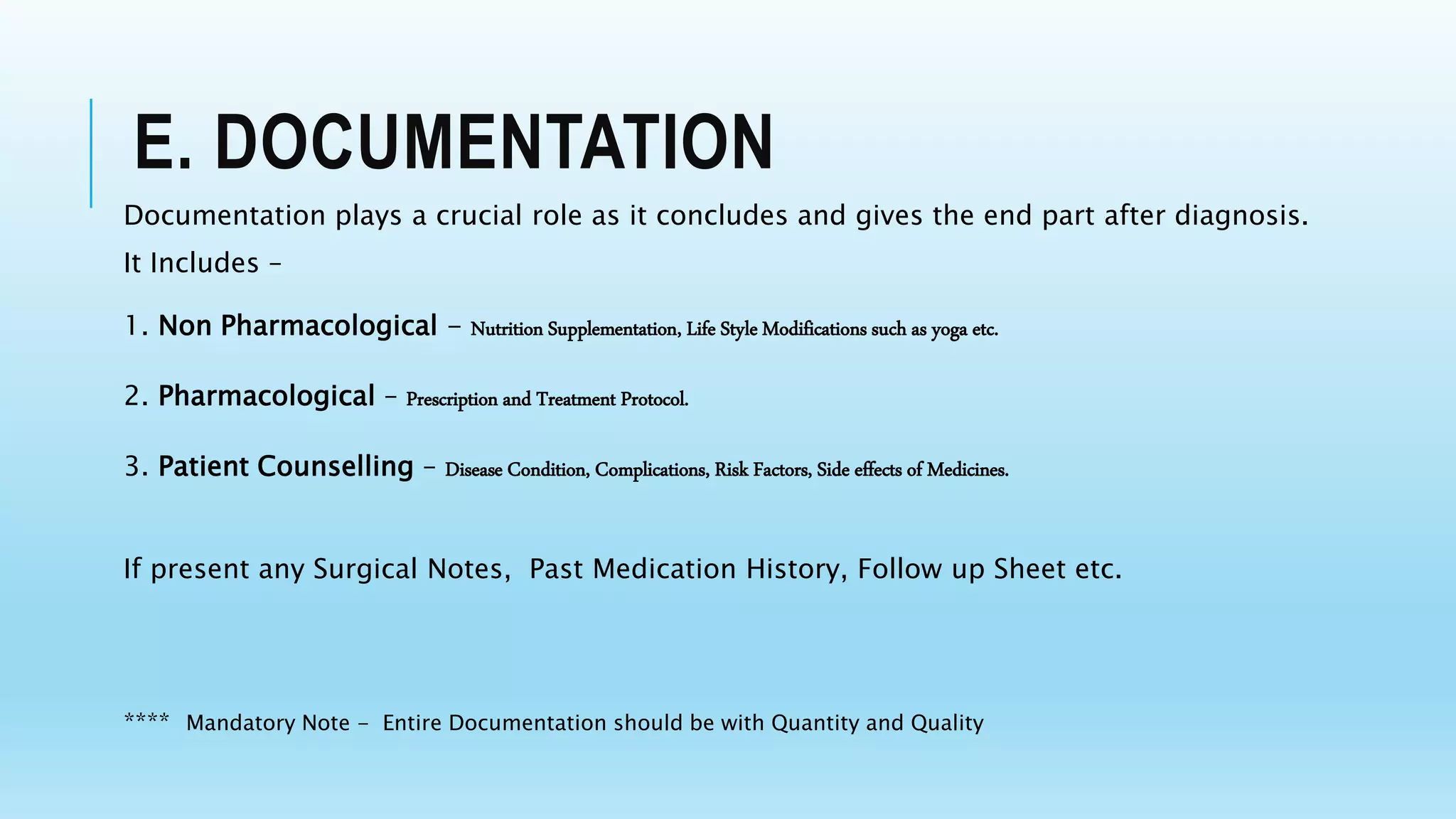


This document outlines important terms and criteria for different types of medical documentation forms. It discusses the key elements that should be included in documentation, such as the chief complaint, history of present illness, review of systems, and past/family history. It also describes different levels of complexity in patient cases and the types of decision making and documentation required. The goal of medical documentation is to comprehensively yet efficiently record all relevant health information about a patient.




























![Evaluation_and_Management[1]](https://cdn.slidesharecdn.com/ss_thumbnails/8209e160-4c89-43f5-bde3-1a2ee8242cc6-150226150420-conversion-gate01-thumbnail.jpg?width=640&height=640&fit=bounds)

































