Downloaded 23 times
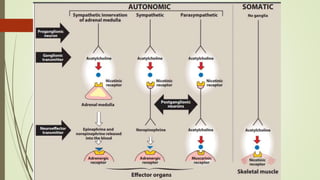

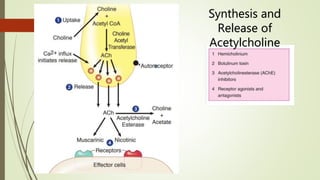
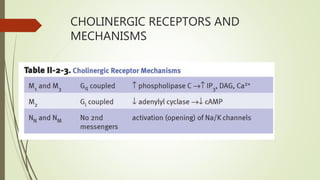
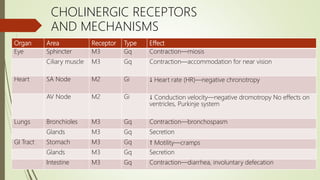
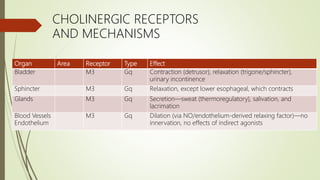
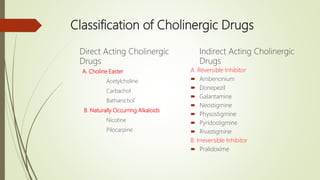
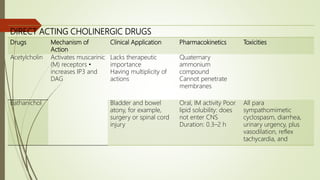
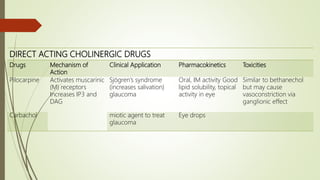
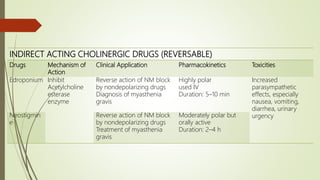
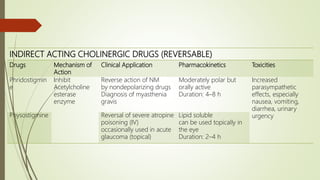
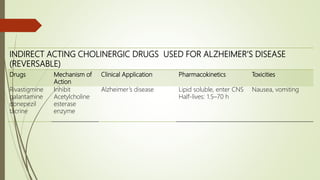
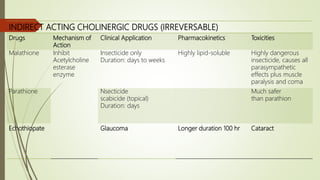
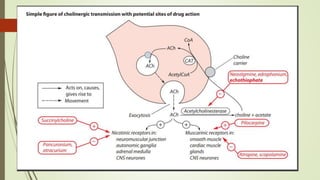

This document discusses the cholinergic autonomic nervous system. It describes the synthesis and release of acetylcholine as well as cholinergic receptors and their effects in different organ systems. It also discusses the classification and mechanisms of direct and indirect acting cholinergic drugs, including their clinical applications and toxicities.





























































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)





