Download as ODP, PPTX









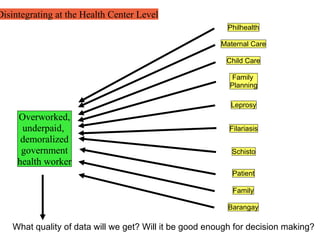







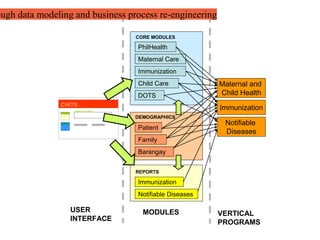














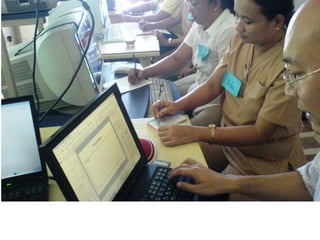












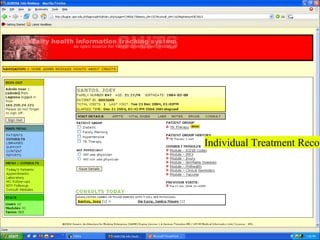
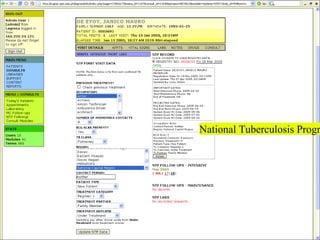










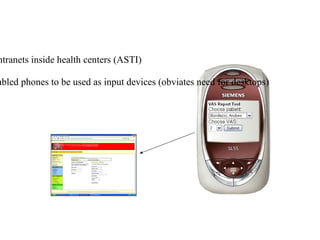

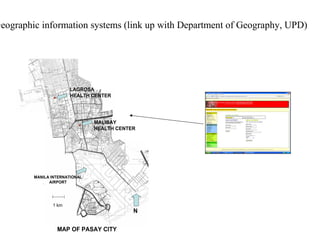
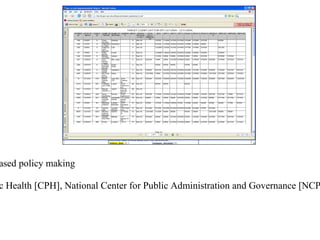



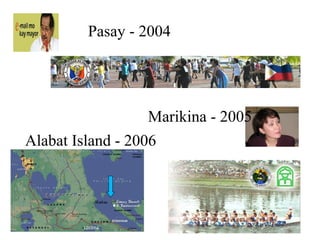





The document introduces the Community Health Information Tracking System (CHITS), an open-source health information system developed to address problems with the Philippines' existing paper-based system. CHITS aims to improve data quality, integrate vertical health programs, and provide faster access to patient records. It was developed through collaboration between health workers and developers to build morale and allow for participation. The system utilizes basic computer hardware and free software to create an affordable solution. It has been piloted in multiple localities and shows benefits like more efficient data management and analysis to help decision making. Future directions may include connecting the system to cellphones and developing additional analytic tools.













































































