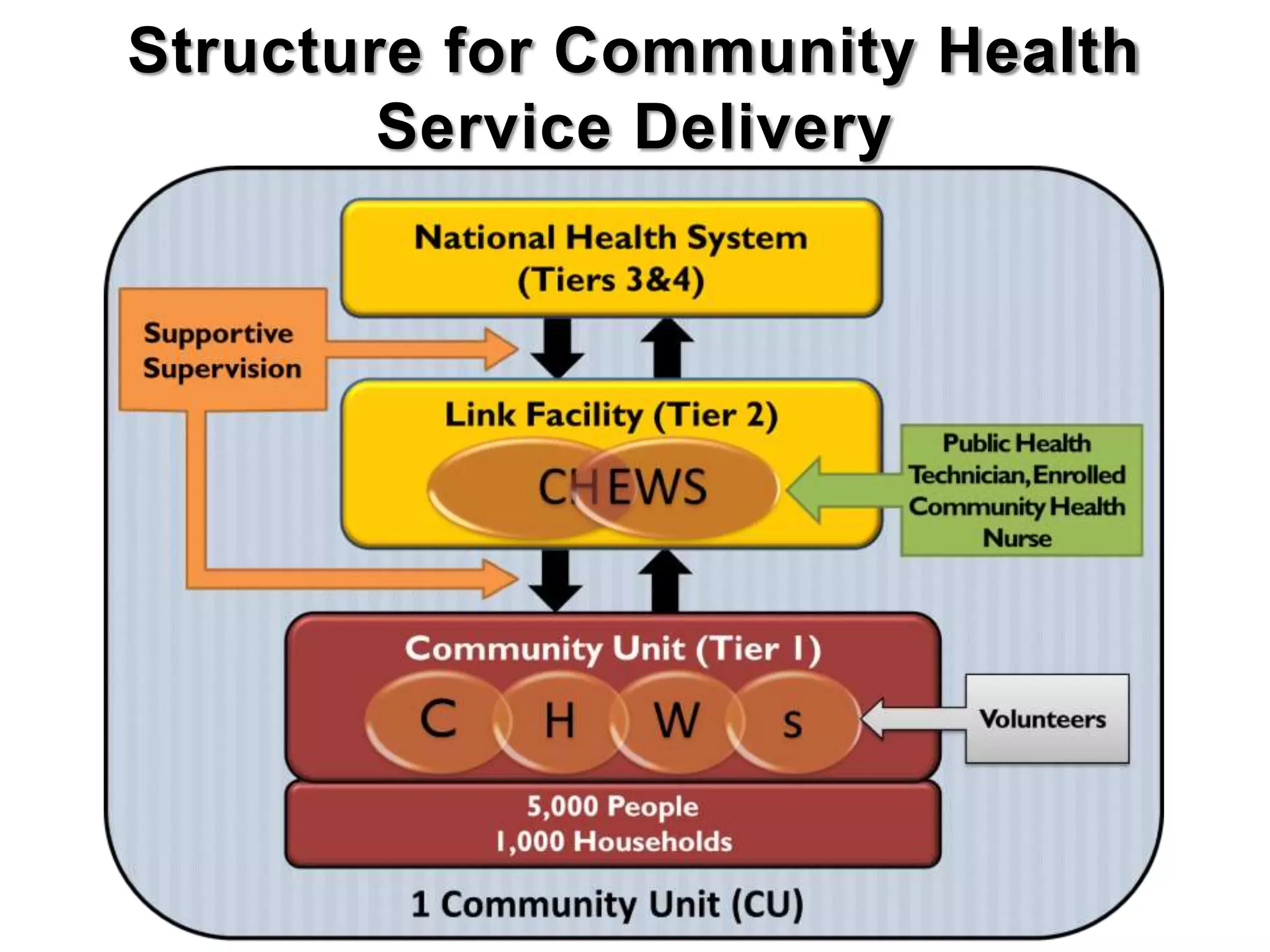
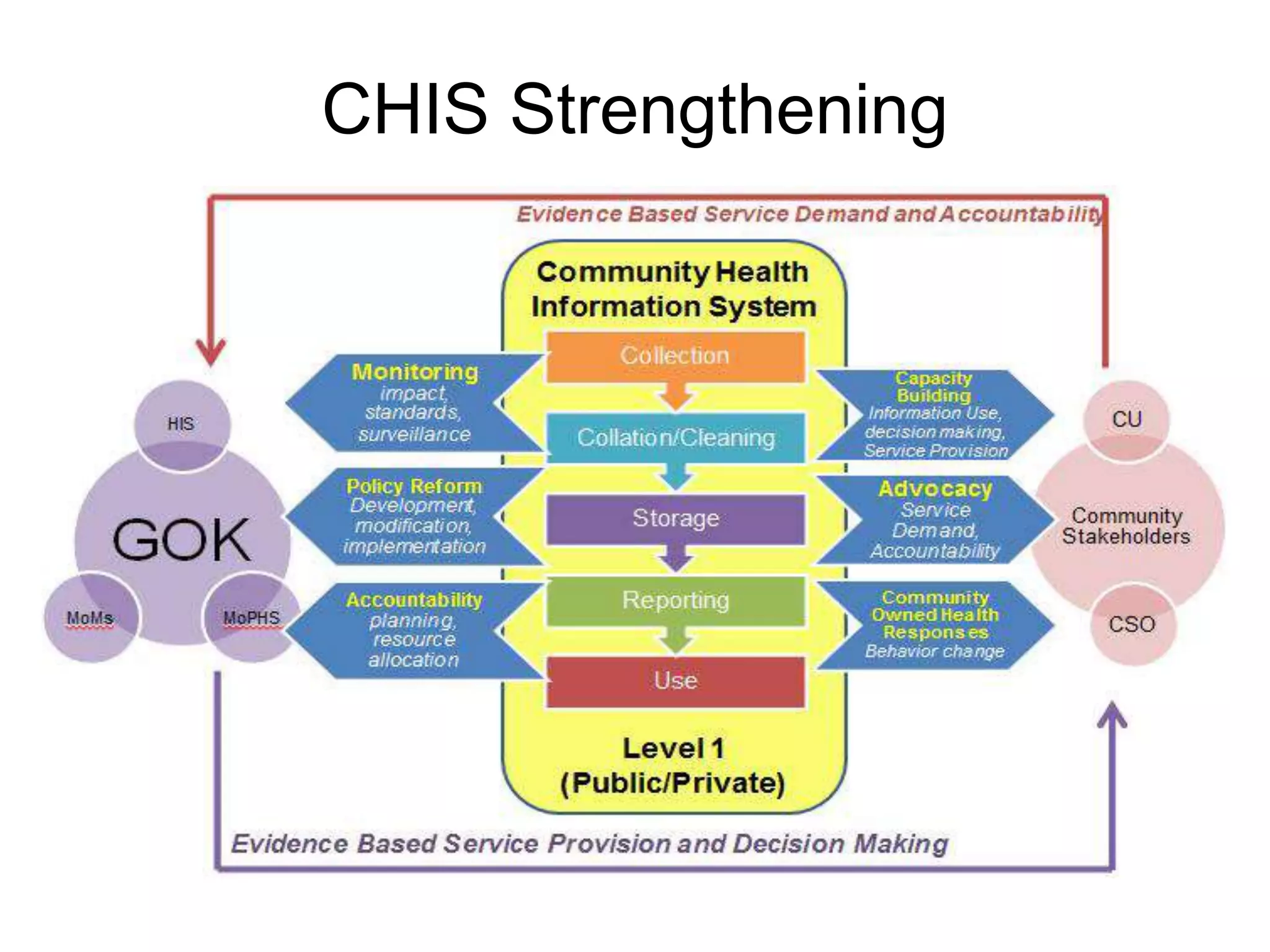
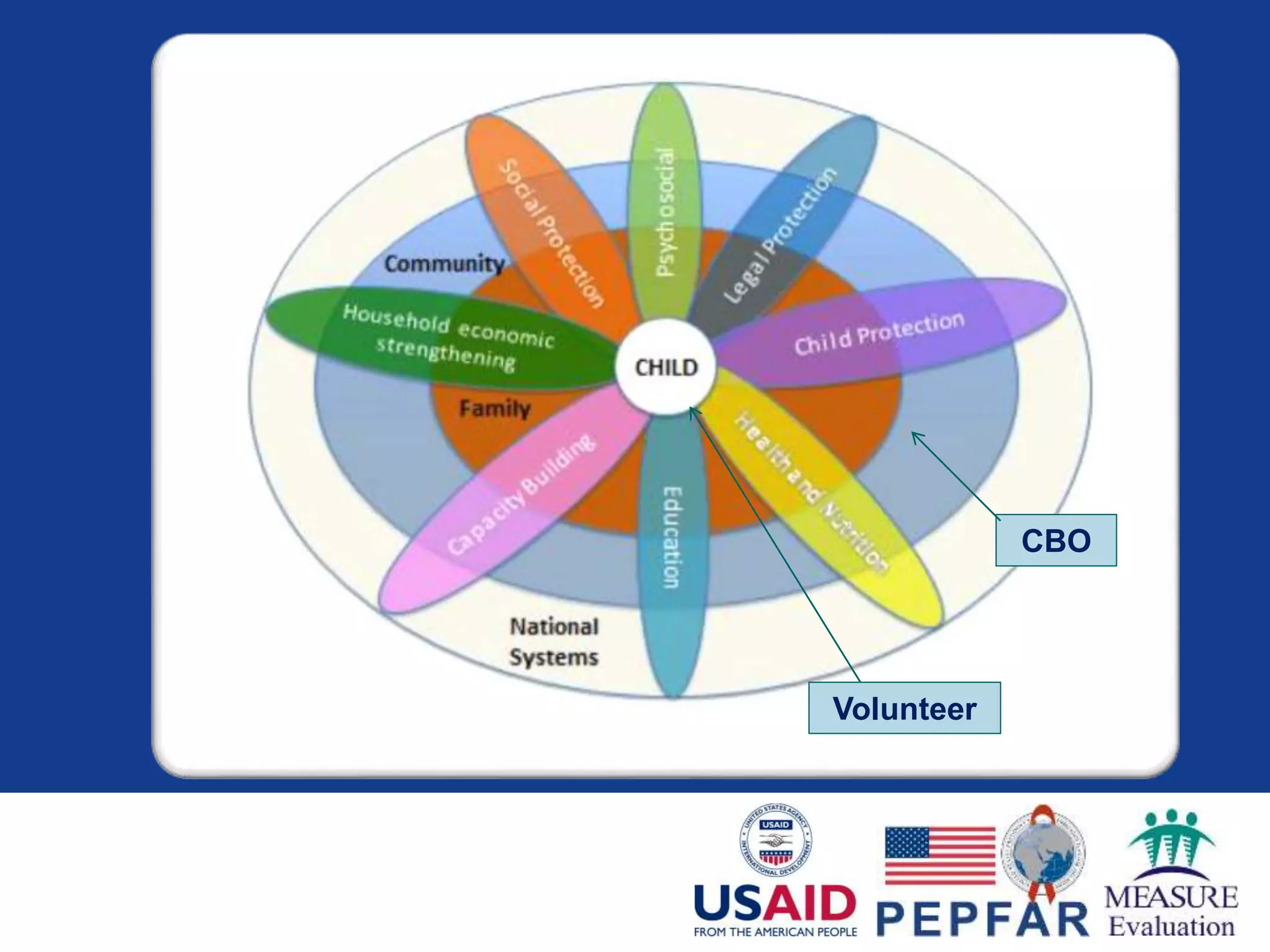
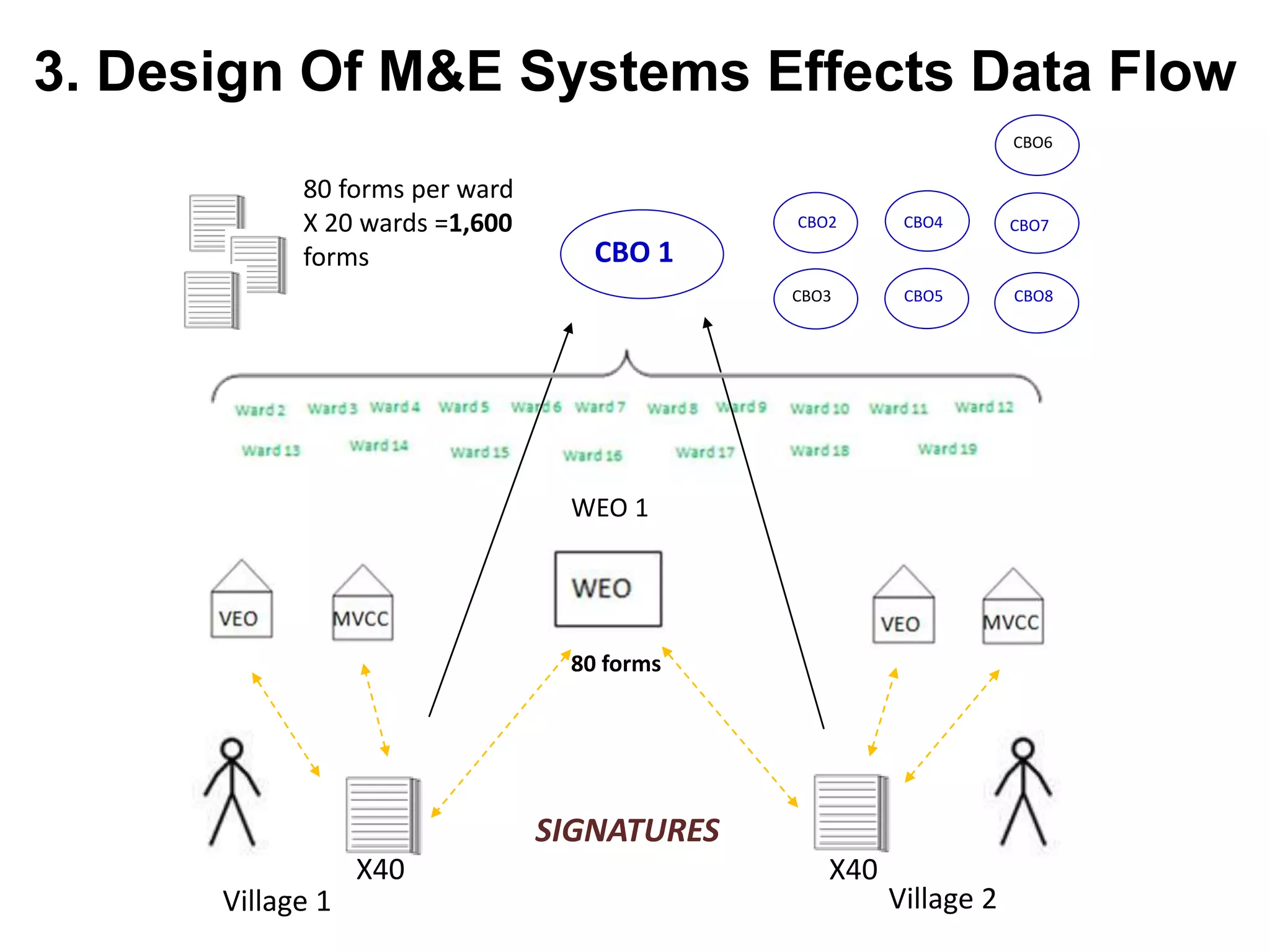
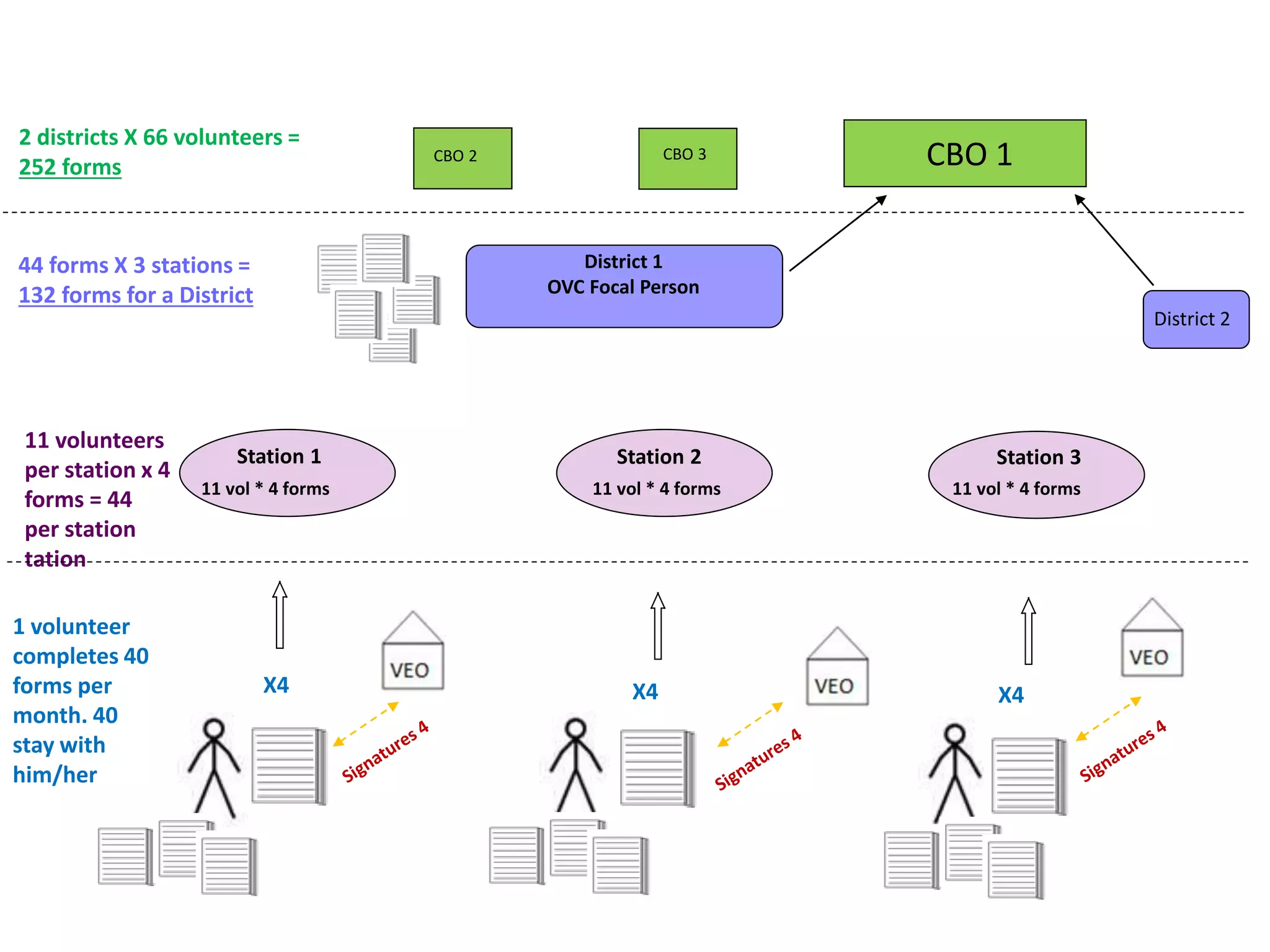
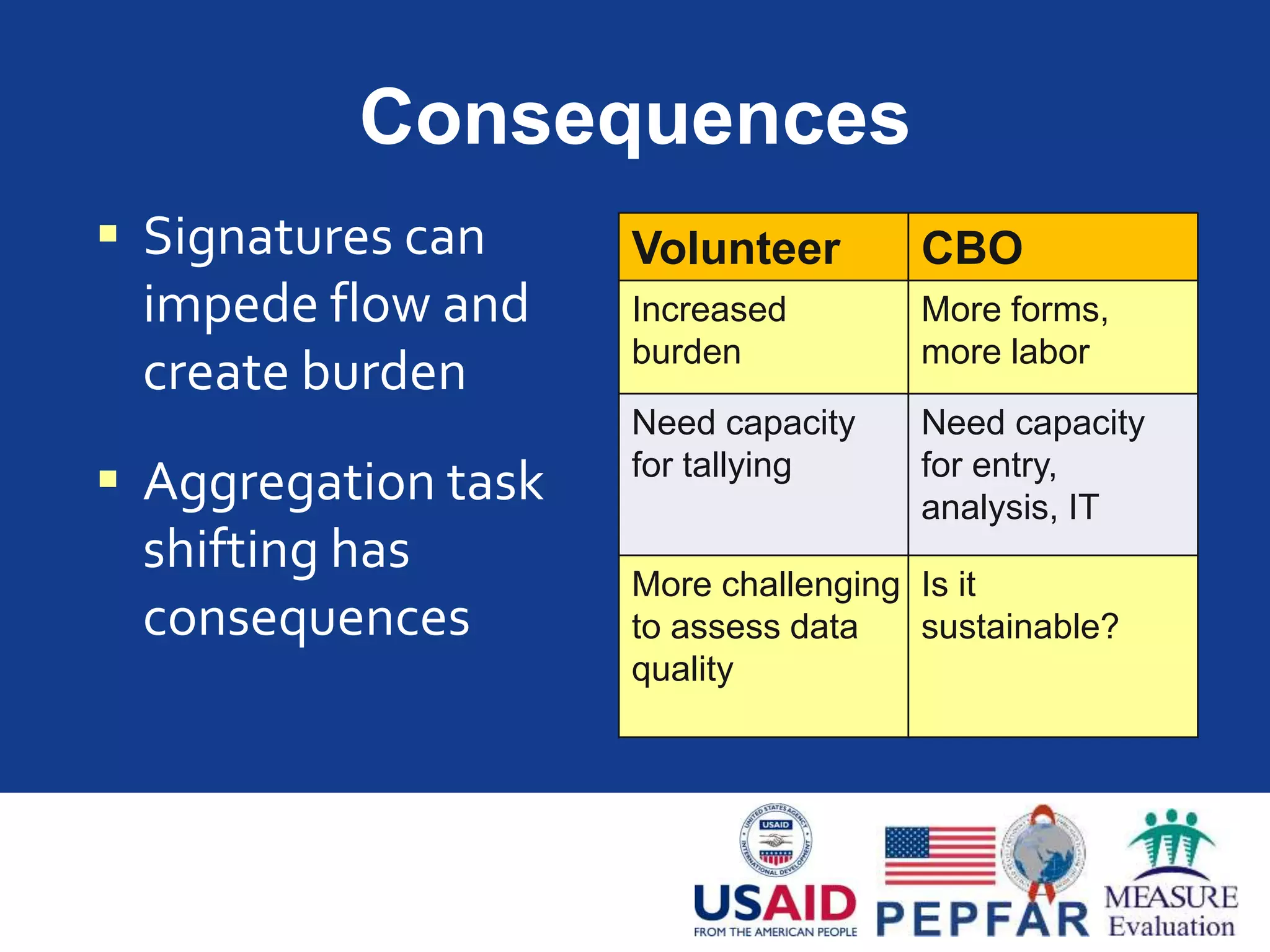
The document discusses building information systems for community programs, focusing on the role of community actors and the importance of quality data in health service delivery and management. It outlines the community health strategy in Kenya and highlights lessons learned regarding monitoring and evaluation, emphasizing that community health information systems require long-term commitment to function effectively. Additionally, it addresses challenges faced in data collection and management, particularly among community-based organizations working with vulnerable populations.