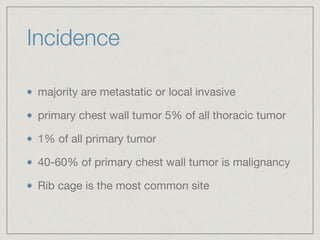
- Primary chest wall tumors account for 5% of all thoracic tumors, with 40-60% being malignant. The rib cage is the most common site.
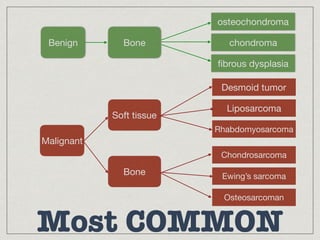
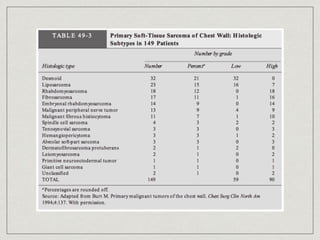
- Common primary bone tumors of the chest wall include osteochondroma, chondroma, fibrous dysplasia, chondrosarcoma, Ewing's sarcoma, and osteosarcoma. Common primary soft tissue tumors include desmoid tumors, soft tissue sarcomas, hemangiomas, and neurofibromas.
- Diagnosis involves imaging like CT, MRI, PET-CT and tissue biopsy. Surgical resection is the main treatment for primary chest wall neoplasms and reconstruction is needed for large defects. Prognosis depends