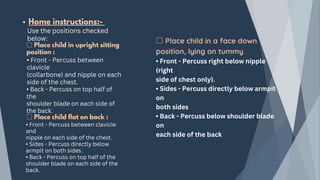
The document outlines chest physiotherapy (CPT), detailing its definition, purposes, indications, techniques, equipment, contraindications, and the nursing role in its implementation and monitoring. CPT is essential for improving respiratory function and mucus clearance in patients with various lung conditions, employing techniques like deep breathing, percussion, and postural drainage. It emphasizes the importance of individualized treatment and the potential complications associated with the procedure, making effective nursing interventions crucial for patient outcomes.