This document provides an overview of radiation protection principles in nuclear medicine based on a chapter from an IAEA publication. It discusses key topics including:
- The ICRP system of radiation protection including principles of justification, optimization and dose limitation.
- Radiation protection quantities such as equivalent dose, effective dose and committed dose quantities.
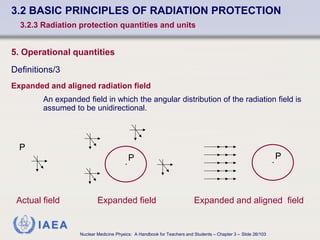
- Operational quantities used for radiation monitoring like ambient dose equivalent and personal dose equivalent.
- International safety standards established by organizations like the IAEA, ICRP and UNSCEAR which are based on balancing radiation risks and benefits.
The document outlines the radiation protection framework and considerations for ensuring safe use of radiation in nuclear medicine facilities.








![IAEA
Nuclear Medicine Physics: A Handbook for Teachers and Students – Chapter 3 – Slide 14/103
3.2 BASIC PRINCIPLES OF RADIATION PROTECTION
3.2.3 Radiation protection quantities and units
1. Mean tissue or organ dose, DT
DT =
εT
mT
Total energy imparted by radiation to that tissue or organ
Mass of the tissue or organ T
SI (International System of Units) unit :
[ DT ] =
1 Joule
1 kilogram
= 1 Gray (Gy)](https://image.slidesharecdn.com/chapter03-221009063035-403ab153/85/Chapter_03-_Radiation_Protection-pdf-14-320.jpg)


![IAEA
Nuclear Medicine Physics: A Handbook for Teachers and Students – Chapter 3 – Slide 17/103
3.2 BASIC PRINCIPLES OF RADIATION PROTECTION
3.2.3 Radiation protection quantities and units
2. Equivalent dose, HT
SI (International System of Units) unit :
[ HT ] =
1 Joule
1 kilogram
= 1 sievert (Sv)](https://image.slidesharecdn.com/chapter03-221009063035-403ab153/85/Chapter_03-_Radiation_Protection-pdf-17-320.jpg)