Downloaded 32 times



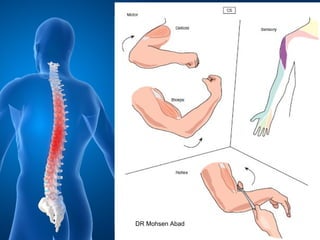
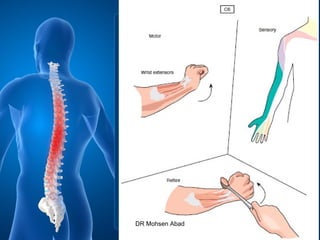
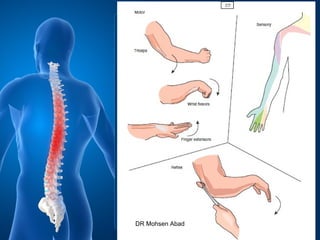
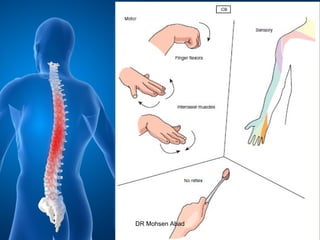








Cervical radicular pain is characterized by upper limb pain due to irritation of cervical spinal nerves, distinct from cervical radiculopathy, which includes neurological deficits. Diagnosis relies on clinical history, examination, and specific tests, with imaging like MRI used to rule out other conditions. Treatment options include conservative management with medications and rehabilitation, interventional techniques like epidural corticosteroid injections, and surgery for severe cases with spinal cord compression.



































































