Download to read offline


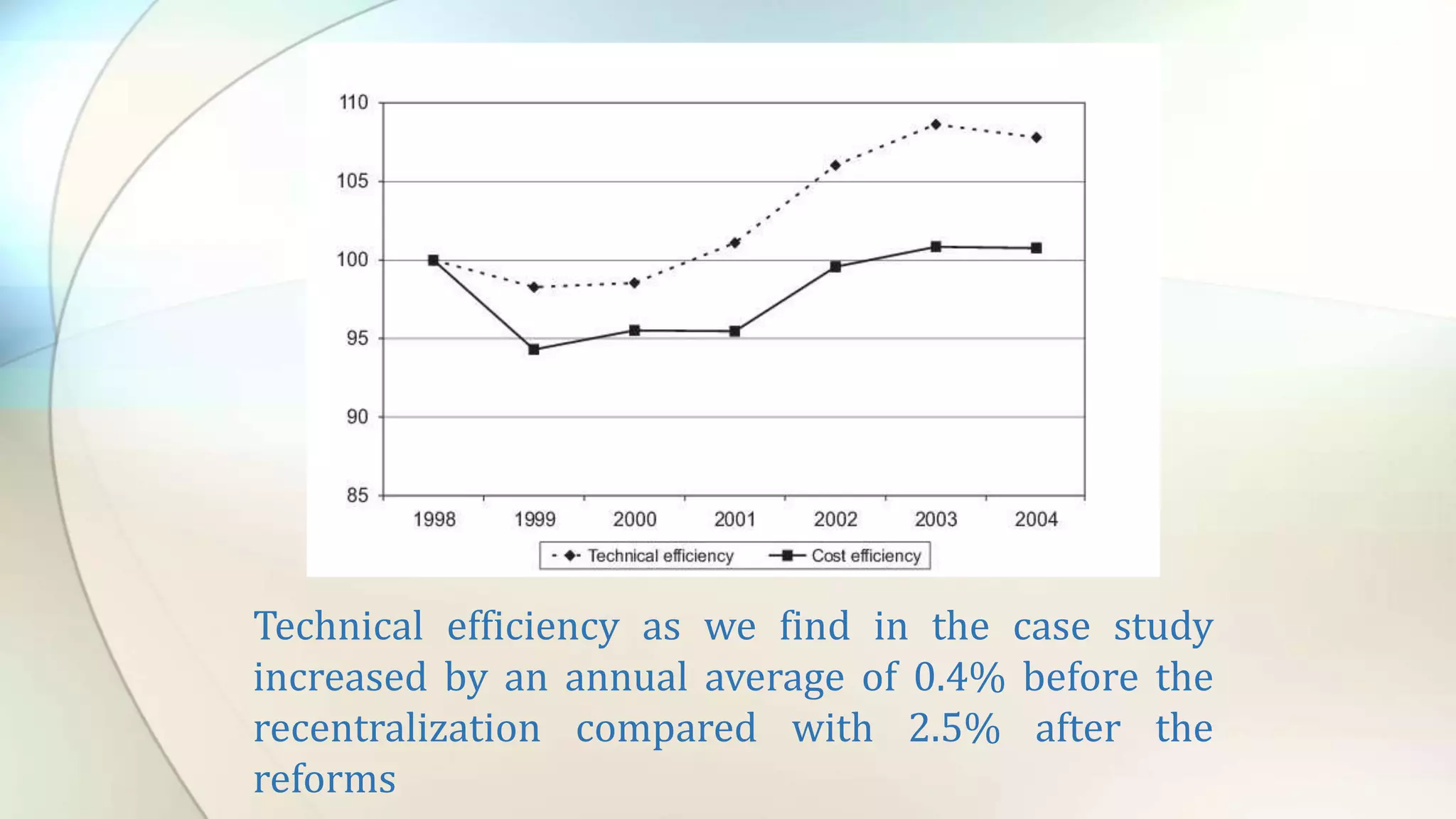
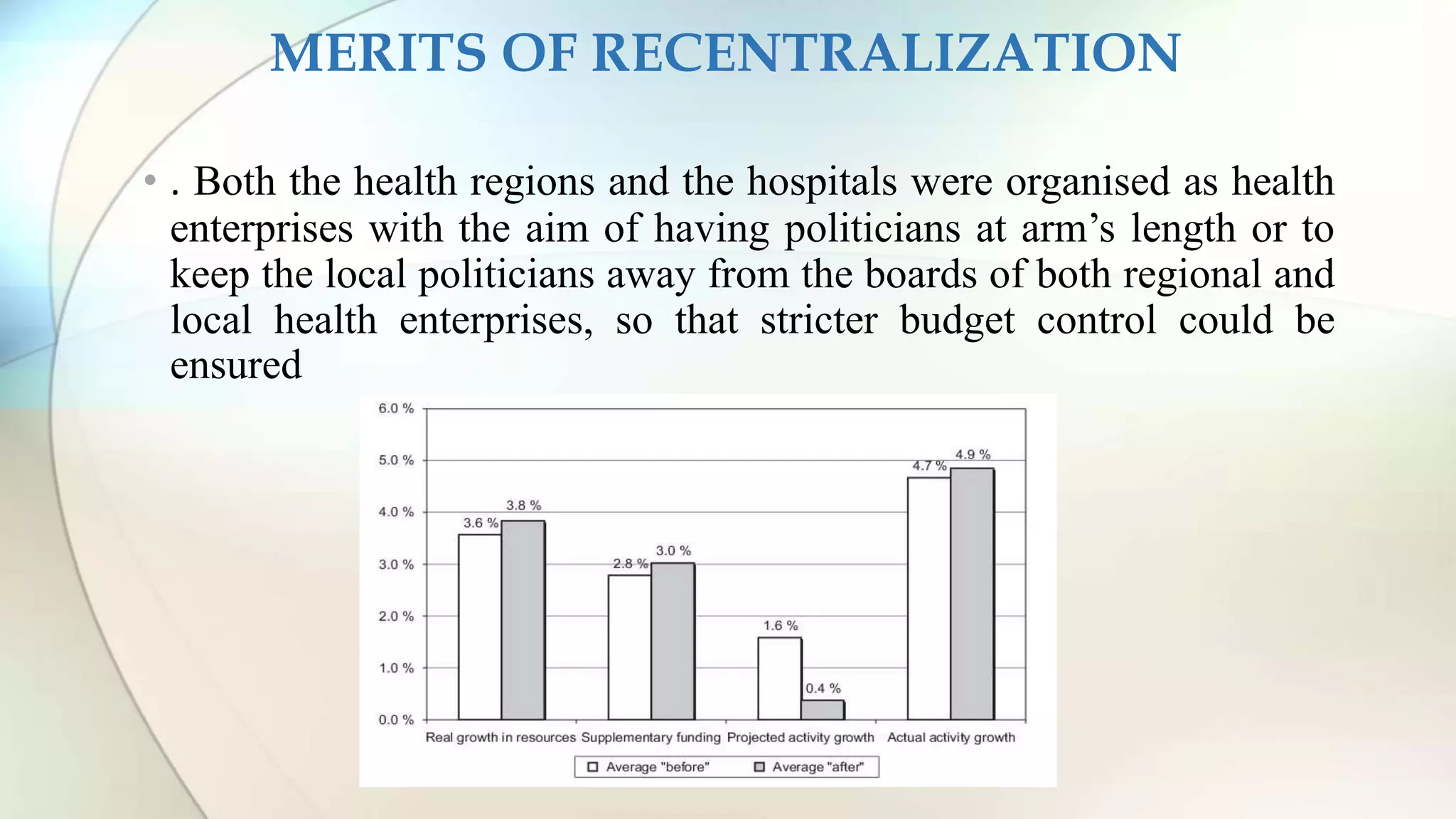


Centralized or Decentralized? A Case study of Norwegian hospital reform analyzes Norway's hospital reforms of 2002 that centralized management of hospitals. The reforms aimed to improve technical efficiency and reduce deficits. While technical efficiency did increase after recentralization, from 0.4% annually to 2.5%, the reforms did not achieve cost containment or reduction in budget deficits as demand decisions remained local and extra funding was provided. Overall, the case study concludes that recentralization is not an effective strategy on its own to control healthcare costs.