Celiac Disease
• Celiacdisease is an autoimmune disorder triggered by gluten.
• Affects approximately 1% of the population but is underdiagnosed.
• Important for Family Medicine physicians to recognize early signs.
4.
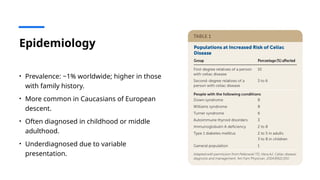
Epidemiology
• Prevalence: ~1%worldwide; higher in those
with family history.
• More common in Caucasians of European
descent.
• Often diagnosed in childhood or middle
adulthood.
• Underdiagnosed due to variable
presentation.
5.
Pathophysiology
• Ingestion ofgluten triggers an immune response.
• Anti-TTG (Anti-tissue Transglutaminase/Anto-EMA
(AntiEndomysial) Antibodies
• Damage to small intestinal villi (villous atrophy).
• Jejunum us Most affected
• Malabsorption of nutrients.
• Involves genetic predisposition (HLA-DQ2, HLA-
DQ8).
6.
Risk Factors
• First-degreerelative with celiac disease.
• Type 1 diabetes.
• Autoimmune thyroid disease.
• Down syndrome, Turner syndrome.
Case Presentation
• History:38-year-old woman with chronic fatigue, iron deficiency anemia, and
intermittent bloating.
• Exam: Mild pallor, no significant findings.
• Labs: CBC shows microcytic anemia; low ferritin.
• Next steps?
10.
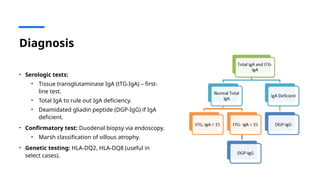
Diagnosis
• Serologic tests:
•Tissue transglutaminase IgA (tTG-IgA) – first-
line test.
• Total IgA to rule out IgA deficiency.
• Deamidated gliadin peptide (DGP-IgG) if IgA
deficient.
• Confirmatory test: Duodenal biopsy via endoscopy.
• Marsh classification of villous atrophy.
• Genetic testing: HLA-DQ2, HLA-DQ8 (useful in
select cases).
11.
Recommendation
• It isrecommended to co-test in all new DM 1 diagnosis (Strong Association)
Role of theFamily Medicine Physician
• Recognize early and atypical presentations.
• Order appropriate screening tests.
• Educate patients about dietary changes.
• Address nutritional deficiencies.
• Iron, B12, Folate, Vitamin D, Calcium, Magnesium, Zinc, Etc…
• Remember Levothyroxine may not be absorbed as well…
• Monitor adherence and refer if needed.
Follow-Up & Long-TermCare
• Annual follow-up for symptoms, adherence, and nutritional status.
• Repeat tTG-IgA levels.
• Bone density screening in high-risk patients.
• Psychological support for dietary changes.
18.
Summary
• Celiac diseaseis often underdiagnosed in primary care.
• Classic and atypical presentations exist.
• Diagnosis via serology and biopsy.
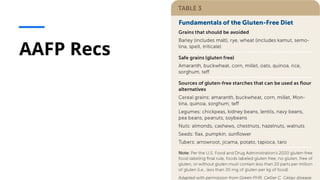
• Strict gluten-free diet is the cornerstone of treatment.
• Family Medicine physicians play a key role in screening, initial management, and follow-
up.
Zonulin and IntestinalPermeability
• What is Zonulin?
• A protein that modulates intestinal permeability by regulating tight junctions between
enterocytes.
• Role in Celiac Disease:
• Increased zonulin levels lead to greater intestinal permeability.
• Allows gluten peptides to cross the epithelial barrier, triggering an immune response.
• Discovery:
• Identified by Dr. Alessio Fasano as a critical factor in the pathogenesis of celiac disease.
21.
Therapeutic Approaches TargetingZonulin
• Zonulin Inhibitors:
• Larazotide acetate (AT-1001): A drug in clinical trials that tightens intestinal junctions to
prevent gluten peptide leakage.
• Shown to reduce symptoms and inflammation in celiac patients.
• Potential Benefits:
• May allow better symptom control even with minimal gluten exposure.
• Could serve as an adjunct to a gluten-free diet.
22.
Emerging Therapeutic Research
•IMU-856:
• A novel small-molecule drug promoting gut barrier integrity.
• Early trials suggest improved nutrient absorption and reduced damage from gluten exposure.
• Enzyme Therapies:
• Latiglutenase: An oral enzyme therapy designed to break down gluten peptides before they trigger an
immune response.
• Aimed at reducing symptoms in patients with accidental gluten exposure.
• Vaccine Research:
• Nexvax2: An experimental vaccine targeting the immune response to gluten.
• Aims to induce immune tolerance but currently on hold due to trial results.
23.
Future Directions inCeliac Disease Treatment
• Current Challenges:
• Strict gluten-free diet remains the only proven treatment.
• Need for therapies that provide greater flexibility in dietary management.
• Future Research:
• Combining zonulin inhibitors, enzyme therapy, and immune modulation.
• Genetic and microbiome studies to identify additional therapeutic targets.