Downloaded 10 times
![UCP/AL/11/221
E.K SANDAMALI
Allied Health Sciences Unit
Faculty of Medicine
University of Colombo
[Musculoskeletal Module]](https://image.slidesharecdn.com/casepresentation2212-150218063535-conversion-gate01/85/Case-presentation-221-2-sandamail-1-320.jpg)
![UCP/AL/11/221
E.K SANDAMALI
Allied Health Sciences Unit
Faculty of Medicine
University of Colombo
[Musculoskeletal Module]](https://image.slidesharecdn.com/casepresentation2212-150218063535-conversion-gate01/75/Case-presentation-221-2-sandamail-1-2048.jpg)
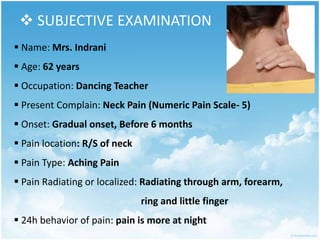
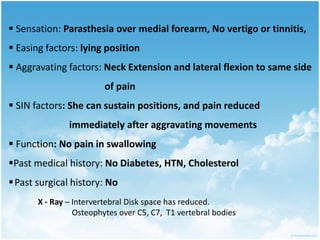
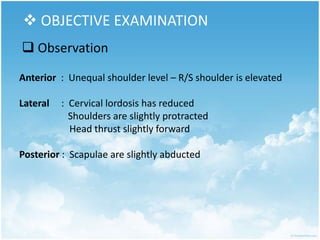
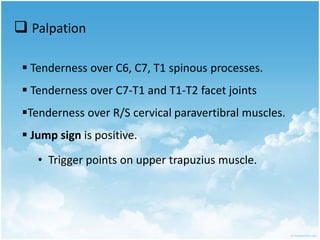
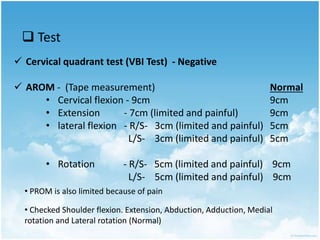

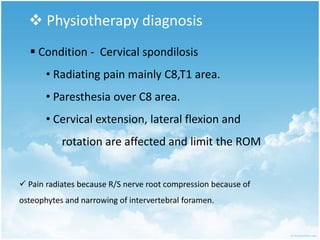

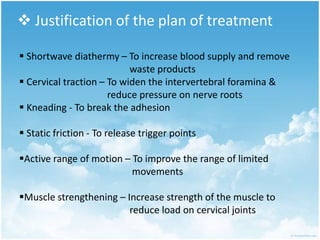
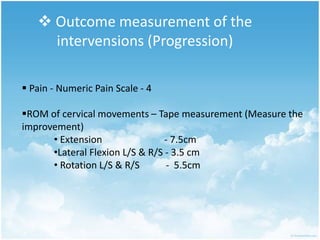


This document contains a physiotherapy assessment and treatment plan for a 62-year-old female presenting with neck pain radiating to her arm. The assessment revealed reduced cervical range of motion, tenderness over the cervical spine, and positive orthopedic tests indicating nerve root compression. X-rays showed reduced disc spaces and osteophytes. The treatment plan includes shortwave diathermy, cervical traction, soft tissue techniques, range of motion exercises, and strengthening to reduce pain and muscle tightness, improve range of motion, and restore normal function. Progress will be measured by pain scale and improved cervical range of motion.












































































