Download as PPS, PPTX



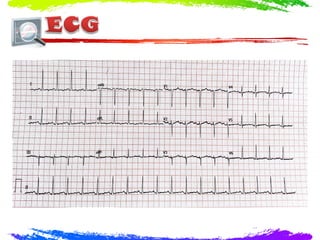
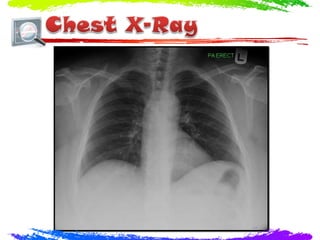
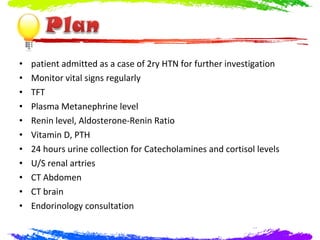
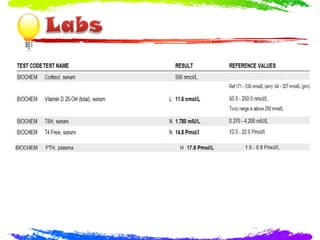
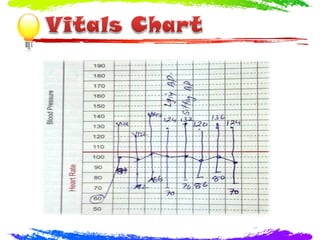


A 28-year-old lady presented with headaches and palpitations for 3 months. On examination, she had a blood pressure of 155/98, heart rate of 117, BMI of 37.6, and fine kinetic tremors with sweaty hands. No significant abnormalities were found on cardiovascular, chest, abdominal, or neurological examinations. She was admitted for further investigation of secondary hypertension. Tests were ordered to evaluate endocrine and renal causes of her high blood pressure. A CT of the brain found evidence of a prior craniotomy but no acute issues.