Download to read offline


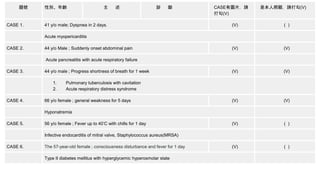

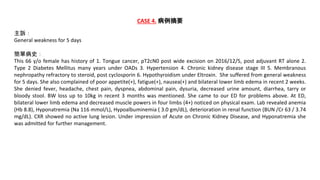
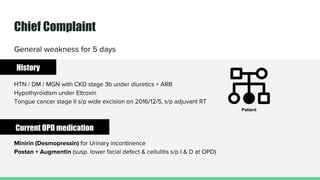
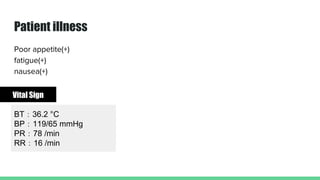
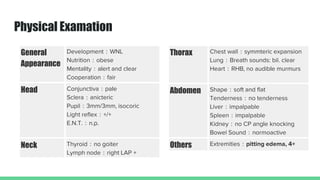

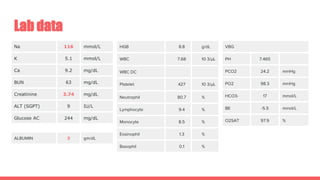
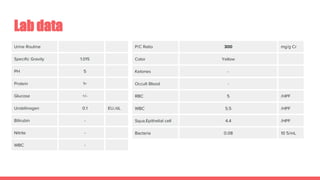
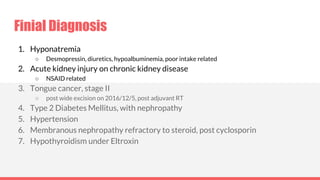

This 66-year-old female presented with general weakness for 5 days. She had a history of tongue cancer, diabetes, hypertension, chronic kidney disease stage 3, and hypothyroidism. On examination, she had bilateral lower limb edema and decreased muscle strength. Laboratory tests showed hyponatremia, hypoalbuminemia, and deteriorated renal function. A chest x-ray was unremarkable. She was diagnosed with acute kidney injury exacerbating her chronic kidney disease, along with hyponatremia likely due to diuretics, desmopressin, and poor oral intake. Her condition improved with fluid restriction and discontinuing medications exacerbating her hypotension.



























































![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)





![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)
